

Trial Conduct, Baseline Characteristics, and Symptom Burden of Patients in the ARISE Study
- PMID: 40198465
- PMCID: PMC12102049
- DOI: 10.1007/s41030-025-00293-3
Trial Conduct, Baseline Characteristics, and Symptom Burden of Patients in the ARISE Study
Abstract
Introduction: ARISE was a global clinical trial designed to generate evidence demonstrating the utility of the patient-reported outcome instruments Quality of Life-Bronchiectasis (QOL-B) [Respiratory Domain (RD) only] and Patient-Reported Outcomes Measurement Information System Short Form v1.0-Fatigue 7a (PROMIS F SF-7a) in patients with newly diagnosed or recurrent Mycobacterium avium complex lung disease (MACLD). Here, we describe trial conduct, patient characteristics, and patient-reported symptoms at baseline among patients enrolled in ARISE.
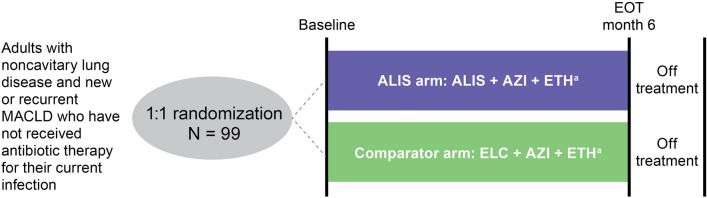
Methods: Adult patients with newly diagnosed or recurrent non-cavitary MACLD who had not initiated antibiotic treatment for their current MAC infection were enrolled; data including comorbidities and prior MACLD history were collected during screening. Symptom burden was assessed using QOL-B, PROMIS F SF-7a, and Functional Assessment of Chronic Illness Therapy (FACIT) questionnaires.
Results: Of 99 patients from 12 countries enrolled in ARISE, the median age was 69.0 years; most were white (80.8%) and female (77.8%). This was the first diagnosis of MACLD for 72.7% of patients. Patients frequently reported having a comorbid respiratory disorder: bronchiectasis (49.5%), asthma (21.2%), and chronic obstructive pulmonary disease (16.2%). At baseline, mean (± SD) and median QOL-B RD scores were 65.0 (± 15.3) and 66.7; PROMIS F SF-7a T-scores were 53.8 (± 8.2) and 55.1; and FACIT-Fatigue scores were 35.0 (± 9.6) and 37.0.
Conclusions: Patients in ARISE were representative of a real-world patient population with MACLD. Comorbid chronic respiratory diseases were common in patients with new or recurrent MACLD, and substantial disease burden at the time physicians initiated MACLD treatment was evidenced by impairment across measures of fatigue and QOL-B domains.
Gov identifier: NCT04677543.
Keywords: Mycobacterium avium complex lung disease; Amikacin liposome inhalation suspension; Clinical trial; Nontuberculous mycobacterial lung disease; Patient-reported outcomes.
Plain language summary
People with a disease called Mycobacterium avium complex lung disease (MACLD) experience many symptoms, including cough, fatigue, and shortness of breath, which can impact their quality of life. It is not clear what symptoms people with new or repeating MACLD may have before they start antibiotic treatment for their disease. This publication describes the design of a study called ARISE, characteristics of people with MACLD who participated, and the symptoms they reported when they started the study. Overall, 99 people with a first, second, or third diagnosis of MACLD, who had not started taking antibiotics, participated in the study. People in the study were on average 69 years old and most were female (78%). This was the first diagnosis of MACLD for more than 70% of people who participated in ARISE. In addition to MACLD, many people also had other respiratory diseases, including bronchiectasis, asthma, and chronic obstructive pulmonary disease. At the start of the study, people completed three questionnaires that measured their symptoms, quality of life, and the severity and frequency of fatigue in their daily life. In these questionnaires, people with MACLD reported that, before starting treatment, they had a high burden of symptoms that impacted their daily lives and quality of life. They also reported more fatigue than people without MACLD. The results from this study were similar to those seen in people with MACLD from registries and other clinical studies. The results also showed that people with MACLD have a large symptom burden before starting treatment.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Charles L. Daley: grant support, advisory board fees, and consulting fees from Insmed Incorporated. Dr. Daley also reports grant support from AN2 Therapeutics, Bugworks, Paratek Pharmaceuticals, Juvabis, FDA, NIH, PCORI, Cystic Fibrosis Foundation, COPD Foundation, and Renovion; advisory board work with AN2 Therapeutics, AstraZeneca, Cepheid, Galapagos, Hyfe, MannKind, Matinas Biopharma, NobHill, Spero Therapeutics, and Zambon; consulting with Galapagos, Genentech, and Pfizer; data monitoring committee work with Otsuka and Bill & Melinda Gates Foundation. James D. Chalmers: grant support from AstraZeneca, Boehringer Ingelheim, Genentech, Gilead Sciences, Grifols, GSK, Trudell, and Insmed Incorporated; consulting fees from Antabio, AstraZeneca, Boehringer Ingelheim, Chiese, Genentech, GSK, Insmed Incorporated, Pfizer, Trudell, and Zambon. Patrick A. Flume: grant support and consulting fees from Insmed Incorporated. David E. Griffith: Consulting fees, personal fees, and advisory board fees from Insmed Incorporated. Dr Griffith also reports consulting and advisory board fees from AN2 Therapeutics and Paratek Pharmaceuticals. Naoki Hasegawa: consulting fees, advisory board fees, and clinical trial design or participation from AN2 Therapeutics and Janssen Pharmaceuticals; consulting fees, advisory board fees, and personal fees from Insmed Incorporated; consulting fees and clinical trial design or participation from MannKind. Kozo Morimoto: consulting fees, personal fees, and advisory board fees from Boehringer Ingelheim and Insmed Incorporated. Kevin L. Winthrop: grant support and consulting fees from AN2 Therapeutics, Insmed Incorporated, MannKind, Paratek Pharmaceuticals, Renovion, and Spero Therapeutics. Korkut Avsar: personal fees from Insmed Incorporated. Luigi Ruffo Codecasa: consulting fees from Cepheid and Dia Sorin. Chau-Chyun Sheu and Dario Andrisani have nothing to report. Dayton W. Yuen, Mariam Hassan, Marie-Laure Nevoret, and Kevin Mange are employees and shareholders in Insmed Incorporated. Charles L. Daley, James D. Chalmers, Patrick A. Flume, David E. Griffith, Naoki Hasegawa, Kozo Morimoto, Kevin L. Winthrop, Luigi Ruffo Codecasa, Chau-Chyun Sheu, Korkut Avsar, and Dario Andrisani were investigators in the ARISE trial. Ethical Approval: A data monitoring committee periodically monitored the safety of patients in the study. ARISE was approved by the Advarra Institutional Review Board under protocol reference number Pro00045468 on 12 August 2020. ARISE also received ethics approval from all study sites. Participants and/or their legally authorized representative were informed that their participation was voluntary. Participants or their legally authorized representative were required to sign a statement of informed consent that met the requirements of 21 CFR 50, local regulations, ICH guidelines, HIPAA requirements. Participants did not consent for publication as no individual patient data are included. ARISE was conducted in compliance with its protocol and the ethical principles derived from international guidelines (Declaration of Helsinki, the Council for International Organizations of Medical Sciences International Ethical Guidelines), and applicable International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use Good Clinical Practice Guidelines, as well as applicable local laws and regulatory requirements.
Figures

References
-
- Hwang JA, et al. Natural history of Mycobacterium avium complex lung disease in untreated patients with stable course. Eur Respir J. 2017;49(3):1600537. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
