

Health-related quality of life in patients with unresectable hepatocellular carcinoma treated with SIRT and nivolumab: a sub-analysis of the NASIR-HCC trial
- PMID: 40198533
- PMCID: PMC11978598
- DOI: 10.1186/s41687-025-00873-6
Health-related quality of life in patients with unresectable hepatocellular carcinoma treated with SIRT and nivolumab: a sub-analysis of the NASIR-HCC trial
Abstract
Background: The health-related quality of life (HRQoL) impact of therapies for hepatocellular carcinoma (HCC) influences decision-making and treatment outcomes. The present study reports HRQoL results from NASIR-HCC, a single-arm study of selective internal radiation therapy (SIRT) with Y90 resin microspheres followed by nivolumab for unresectable HCC.
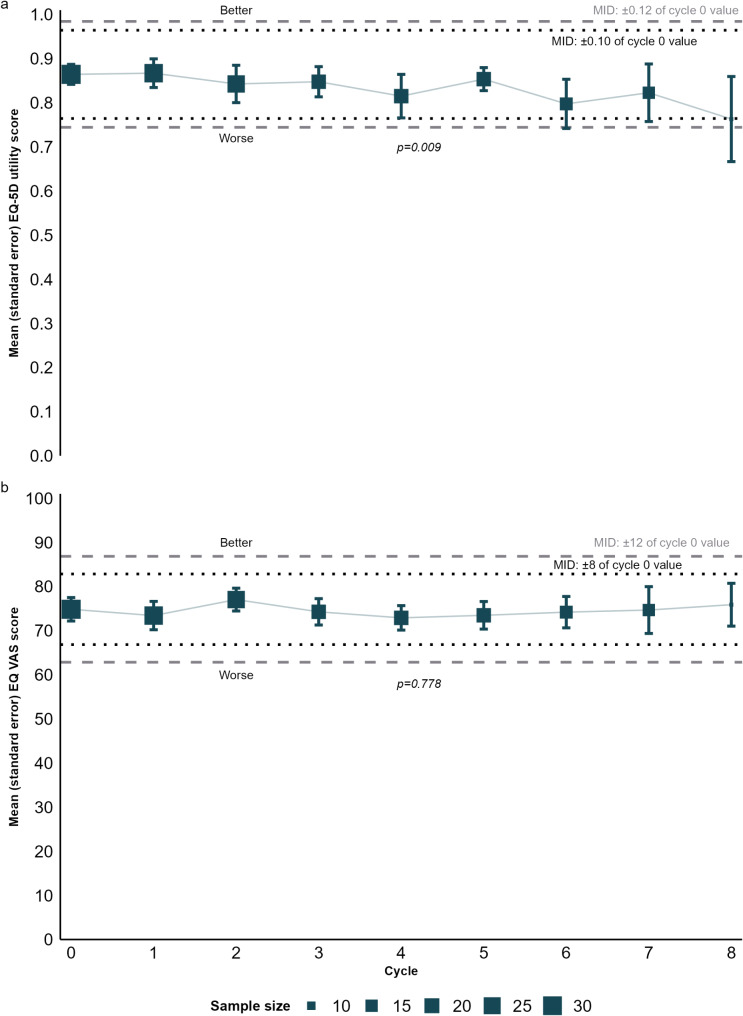
Methodology: Participants completed the EQ-5D-3 L, EQ-VAS, and FACT-Hep at baseline and on the first day of each nivolumab cycle. Linear mixed-effect models were used to calculate changes in outcomes in participants with the baseline and ≥ 1 follow-up measurement. Changes were assessed for clinical meaningfulness versus published minimally important differences.
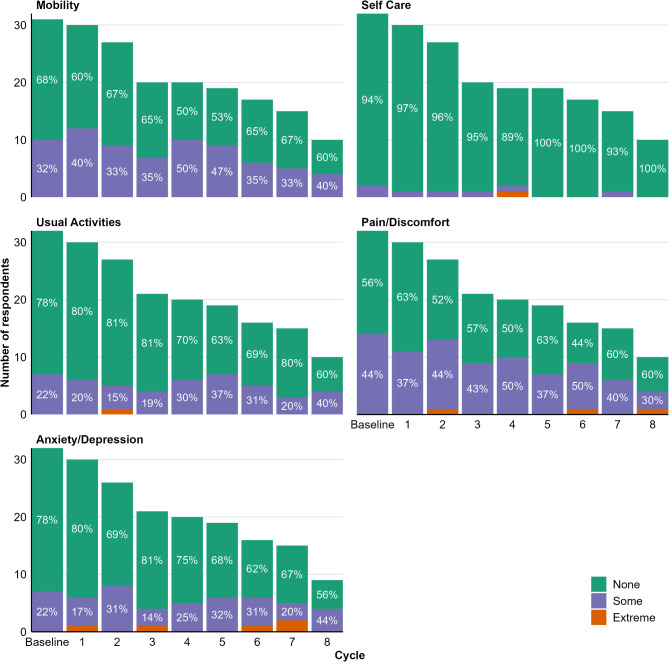
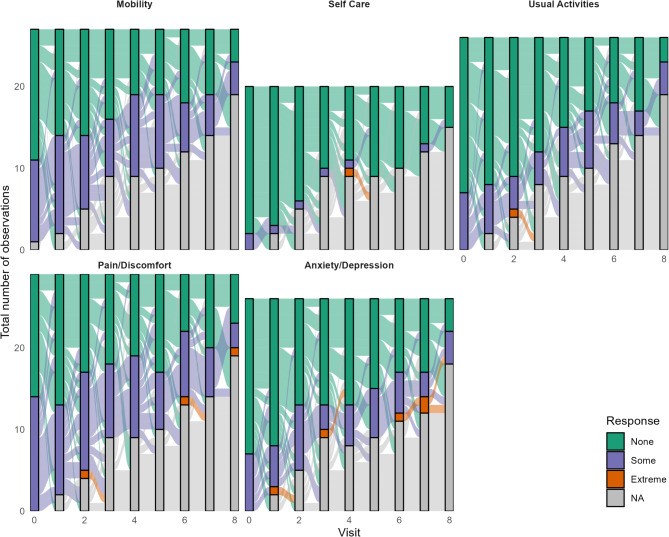
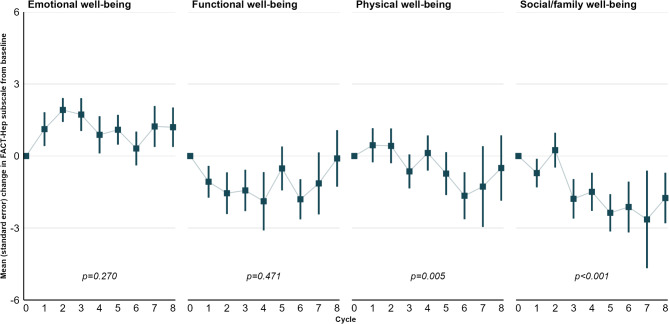
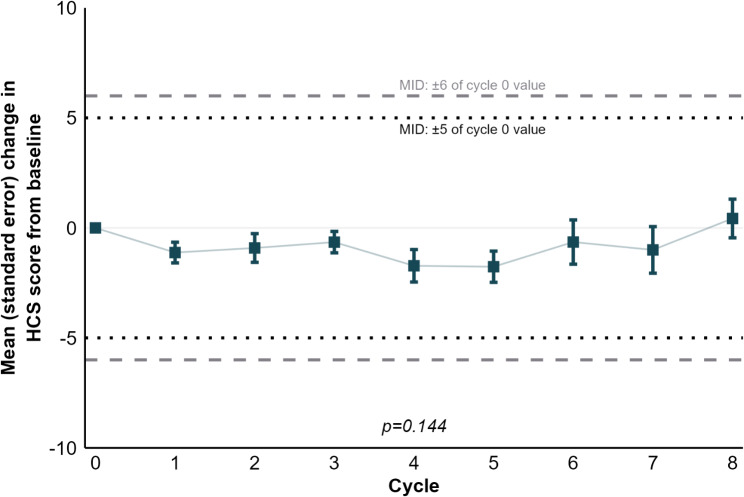
Results: Thirty-two patients from NASIR-HCC were included. Completion rates exceeded 70% at 62% of time points. Across EQ-5D-3 L domains, minimal changes were reported. Most patients had no problems at almost all time points. Mean index values were 0.864 at baseline and 0.763 in cycle 8, but this difference was not clinically meaningful. The small EQ-VAS increase, from 74.8 at baseline to 75.9 in cycle 8, was also not clinically meaningful. The various FACT scales remained stable, although transient but not clinically meaningful declines occurred for some scales. The median time to deterioration was 5.5 months for the FACT-Hep score.
Conclusions: Combining SIRT with nivolumab did not compromise HRQoL in patients with unresectable HCC. Study results were limited by the small number of patients but, combined with the previously reported clinical outcomes, suggested that the treatment combination deserves further consideration in this difficult-to-treat population.
Trial registration number/date of registration: NCT03380130. First submitted on 2017-10-20; https://clinicaltrials.gov/study/NCT03380130 .
Keywords: Hepatocellular carcinoma; Immunotherapy; Nivolumab; Quality of life; SIR-Spheres; Selective internal radiation therapy.
Plain language summary
Patients with hepatocellular carcinoma often have poor health-related quality of life. Any treatment for hepatocellular carcinoma should aim to, at best, improve health-related quality of life, and, at the very least, prevent further declines. For the novel treatment combination of selective internal radiation therapy with Y90 resin microspheres and the immunotherapeutic drug nivolumab, clinical but no health-related quality of life data have been published before. The present study is the first to provide such data, based on the NASIR-HCC study, in which participants with unresectable hepatocellular carcinoma completed multiple instruments to measure health-related quality of life, including the EQ-5D-3 L and the FACT-Hep questionnaire. For all measurements, scores remained broadly stable over time and where changes were observed, in either a positive or a negative direction, these were transient and not clinically meaningful. These findings imply that selective internal radiation therapy followed by eight cycles of nivolumab does not reduce health-related quality of life in unresectable hepatocellular carcinoma. This treatment combination therefore should be evaluated further for this patient population, in particular as its clinical data have also been promising.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The study was conducted in line with the principles of the Declaration of Helsinki and conducted in accordance with Good Clinical Practice guidelines. The protocol was approved by the ethics committee (Comite Etico de Investigacion Clinica de Navarra, EudraCT: 2017-000232-34, internal code 20/17). Consent to participate: All patients provided written informed consent before study participation. Consent to publish: All authors consent to publish the final manuscript. Competing interests: Manuel de la Torre-Aláez has received travel grants from Bayer, Eisai, Pfizer, and Roche. Ana Matilla has received consultancy fees from AstraZeneca, Bayer, Eisai/MSD, Roche, and Sirtex Medical; travel grants from AstraZeneca, Bayer, and Boston Scientific. María Varela has received lecture, congress participation, and consultancy fees as well as travel grants from AstraZeneca, Boston Scientific, Eisai/MSD, and Roche. Mercedes Iñarrairaegui has received lecture fees and travel grants from Bristol Myers Squibb. María Reig has received consultancy fees from AstraZeneca, Bayer, Bristol Myers Squibb, Boston Scientific, Eli Lilly, Ipsen, and Roche; lecture fees from Bayer, Bristol Myers Squibb, Eli Lilly, Gilead, Roche, and Universal Diagnostics; travel grants from AstraZeneca, Bayer, Bristol Myers Squibb, and Eli Lilly; research grants (to institution) from Bayer and Ipsen. Jose Luis Lledó has received speaker and consultancy fees from AstraZeneca, Bayer, Eisai, MSD, and Roche. Juan Ignacio Arenas declares no financial interest. Sara Lorente declares no financial interest. Milagros Testillano has received travel grants from AbbVie. Laura Márquez has received speaker fees from Bayer, Eisai, and Gilead; advisory fees from Eisai and MSD. Gemma Iserte declares no financial interest. Josepmaria Argemí declares no financial interest. Carlos Gómez-Martin has received consultancy fees from Amgen, AstraZeneca, Bristol Myers Squibb, Eisai, Hengrui Therapeutics, Merck, and Roche Spain; speaker fees from Eisai and Eli Lilly. Macarena Rodríguez-Fraile has received speaker and consultancy fees from Sirtex Medical. Jose I. Bilbao has received consultancy fees from Boston Scientific, MSD, Sirtex Medical, and Terumo; speaker fees from Sirtex Medical; research grants from Sirtex Medical and Terumo. Richard F. Pollock is director at Covalence Research Ltd, which has received consultancy fees from ALK, AstraZeneca, Dexcom, Eli Lilly, Genmab, Janssen, medac, Medtronic, Menarini, Novo Nordisk, Otsuka/Avanir, Pharmacosmos, Roche Diagnostics, Siemens Healthineers/Varian, Sirtex Medical (including for assistance with the preparation of this manuscript), and Y-mAbs. Johannes Pöhlmann is an employee at Covalence Research Ltd, which has received consultancy fees from ALK, AstraZeneca, Dexcom, Eli Lilly, Genmab, Janssen, medac, Medtronic, Menarini, Novo Nordisk, Otsuka/Avanir, Pharmacosmos, Roche Diagnostics, Siemens Healthineers/Varian, Sirtex Medical (including for assistance with the preparation of this manuscript), and Y-mAbs. Ion Agirrezabal was employed by Sirtex Medical when the present study was initiated and conducted and is now employed by Sanofi. Bruno Sangro has received consultancy fees from Adaptimmune, AstraZeneca, Bayer, Bristol Myers Squibb, Boston Scientific, BTG, Eisai, Eli Lilly, H3 Biomedicine, Ipsen, Merck, Novartis, Roche, Sirtex Medical, and Terumo; speaker fees from AstraZeneca, Bayer, Bristol Myers Squibb, BTG, Eli Lilly, Ipsen, Merck, Novartis, Roche, Sirtex Medical, and Terumo; research grants (to institution) from BMS and Sirtex Medical.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
