

Prevalence, trends, and maternal risk factors of adverse birth outcomes from a hospital-based birth defects surveillance system in Kampala, Uganda, 2015-2022
- PMID: 40200189
- PMCID: PMC11980181
- DOI: 10.1186/s12884-025-07550-y
Prevalence, trends, and maternal risk factors of adverse birth outcomes from a hospital-based birth defects surveillance system in Kampala, Uganda, 2015-2022
Abstract
Background: Adverse birth outcomes (ABOs) cause significant infant morbidity and mortality in resource-limited settings. Many of the maternal risk factors associated with ABOs can be prevented. We present the prevalence, trends, and risk factors of selected ABOs from a hospital-based birth defects surveillance program in Kampala, Uganda.
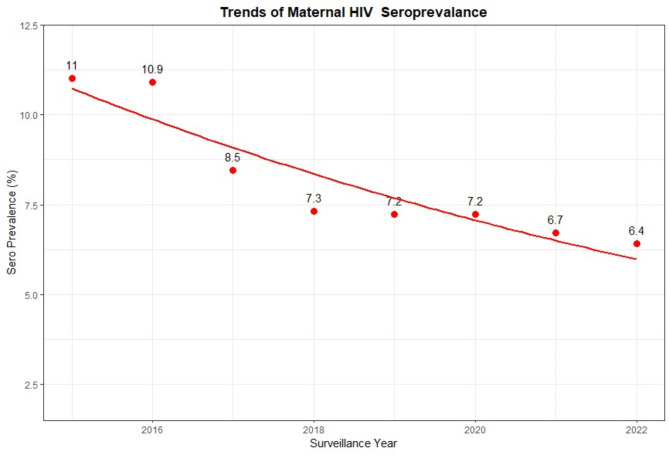
Methods: We analyzed data for all mothers with singleton deliveries collected from four urban hospitals between 2015 and 2022. Prevalence of preterm birth [PTB], low birth weight [LBW], small for gestational age [SGA], and stillbirth [SB] and maternal HIV seroprevalence were calculated among 222,427 births. SB was defined as infant born without life ≥ 28 weeks of gestation, LBW as term live birth weighing < 2500 g and PTB as live birth born < 37 weeks of gestation. Time trends of ABOs by maternal HIV status and age were computed using quasi-Poisson regression model and presented graphically. Risk factor associations were estimated using robust Poisson models adjusting for infant sex, hospital of delivery, and birth year.
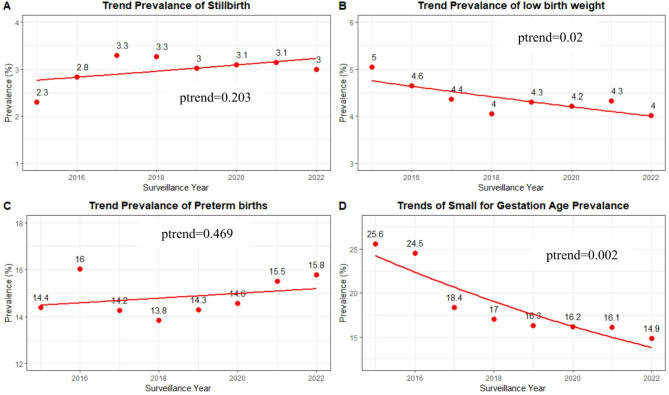
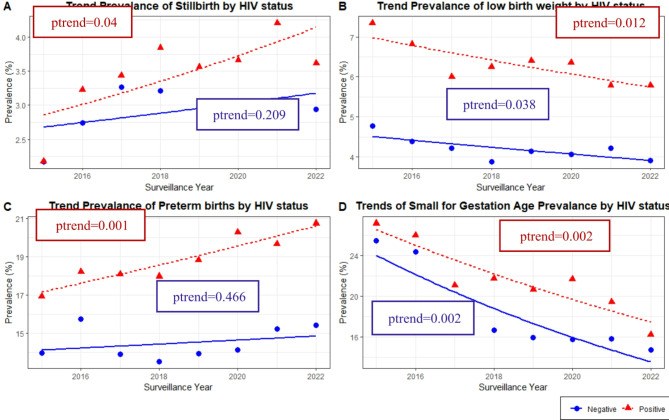
Results: Prevalence of PTB, LBW, SGA, and SB were 14.8%, 4.3%, 17.8%, and 3.1%, respectively. Maternal HIV seroprevalence was 7.7%. Compared to mothers aged 25-34 years, young adolescents 10-18 years was associated with PTB (adjusted risk ratio [aRR]: 1.44, 95% confidence interval (CI): 1.38-1.50); LBW (1.65,1.51-1.81); and SGA (1.18; 1.12-1.24). HIV seropositivity was associated with PTB (1.18; 1.14-1.22), LBW (1.54; 1.43-1.65), and SGA (1.28; 1.23-1.33). Compared to starting ANC in the first trimester, no antenatal care (ANC) was associated with PTB (2.44; 2.33-2.56), LBW (1.80; 1.55-2.09), SGA (1.37; 1.27-1.49), and SB (3.73; 3.32-4.15) and late attendance with LBW (1.09; 1.02-1.16), SGA (1.26; 1.22-1.30), and SB (1.09; 1.02-1.17). Our findings also indicate a rising trend in PTB among adolescent and young women aged 10-24 years, and a declining trend in LBW and SGA over time (ptrend < 0.05 for all).
Conclusions: Young maternal age, maternal HIV, and late or no ANC attendance were associated with ABO. Childbearing in the ages 25-34, preventing HIV in women, and supporting early and frequent ANC attendance are important in improving birth outcomes.
Keywords: Adverse birth outcomes; Low birth weight; Preterm birth; Small for gestational age; Stillbirth.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study and all methods involved were performed in accordance with the ethical principles for medical research involving human subjects, stipulated within the World Medical Association (WMA) declaration of Helsinki. This study was reviewed and approved by the U.S. Centers for Disease Control and Prevention Institutional Review Board (IRB) protocol number #6606, the Joint Clinical Research Center IRB, and the Uganda National Council for Science and Technology (UNCST), following 45 C.F.R. part 46; 21 C.F.R. part 56. Consent to participate in the surveillance was waived by both IRBs (JCRC and CDC) because the surveillance involves no more than minimal risk to the participants. However, IRB-approved written informed consent was obtained for photographs of newborns with birth defects from their mothers or legal guardians. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Disclaimer: The findings and conclusions are those of the authors and do not necessarily represent the official position of the funding agencies.
Figures

Similar articles
-
Correlates and outcomes of preterm birth, low birth weight, and small for gestational age in HIV-exposed uninfected infants.BMC Pregnancy Childbirth. 2014 Jan 8;14:7. doi: 10.1186/1471-2393-14-7. BMC Pregnancy Childbirth. 2014. PMID: 24397463 Free PMC article.
-
Preterm birth and fetal growth restriction in HIV-infected Brazilian pregnant women.Rev Inst Med Trop Sao Paulo. 2015 Mar-Apr;57(2):111-20. doi: 10.1590/S0036-46652015000200003. Rev Inst Med Trop Sao Paulo. 2015. PMID: 25923889 Free PMC article.
-
The prevalence of histologic acute chorioamnionitis among HIV infected pregnant women in Uganda and its association with adverse birth outcomes.PLoS One. 2019 Apr 11;14(4):e0215058. doi: 10.1371/journal.pone.0215058. eCollection 2019. PLoS One. 2019. PMID: 30973949 Free PMC article. Clinical Trial.
-
Risk of stillbirth, preterm delivery, and fetal growth restriction following exposure in a previous birth: systematic review and meta-analysis.BJOG. 2018 Jan;125(2):183-192. doi: 10.1111/1471-0528.14906. Epub 2017 Oct 3. BJOG. 2018. PMID: 28856792
-
Influence of the maternal birth status on offspring: a systematic review and meta-analysis.Acta Obstet Gynecol Scand. 2009;88(12):1307-18. doi: 10.3109/00016340903358820. Acta Obstet Gynecol Scand. 2009. PMID: 19916879
References
-
- Althabe F. Born too soon: the global action report on preterm birth. World Health Organization; 2012.
-
- Lawn JE, et al. Small babies, big risks: global estimates of prevalence and mortality for vulnerable newborns to accelerate change and improve counting. Lancet. 2023;401(10389):1707–19. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
