

More or less equal? Trends in horizontal equity in mental health care utilization in Stockholm county, Sweden (2006-2022). Repeated survey-registry linked studies
- PMID: 40200310
- PMCID: PMC11980088
- DOI: 10.1186/s12939-025-02453-y
More or less equal? Trends in horizontal equity in mental health care utilization in Stockholm county, Sweden (2006-2022). Repeated survey-registry linked studies
Abstract
Background: Horizontal equity is defined as equal care for equal needs, regardless of socioeconomic factors. This study investigated trends in horizontal equity in mental health care (MHC) utilization in Sweden from 2006 to 2022. Monitoring equity provides valuable information for healthcare system governance (e.g., planning and resource allocation) necessary for ensuring equitable provision of services.
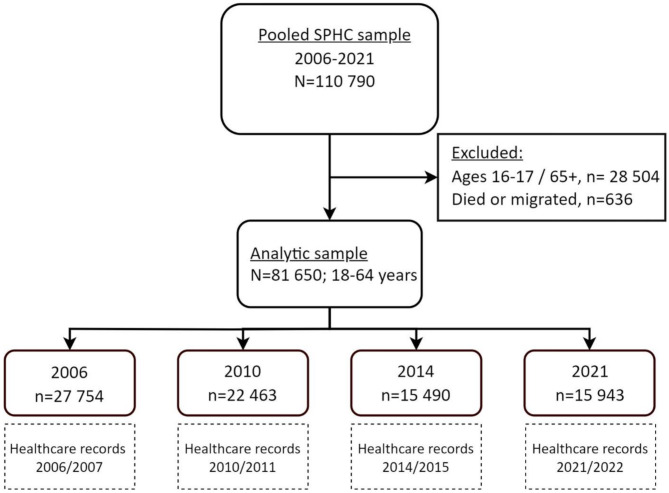
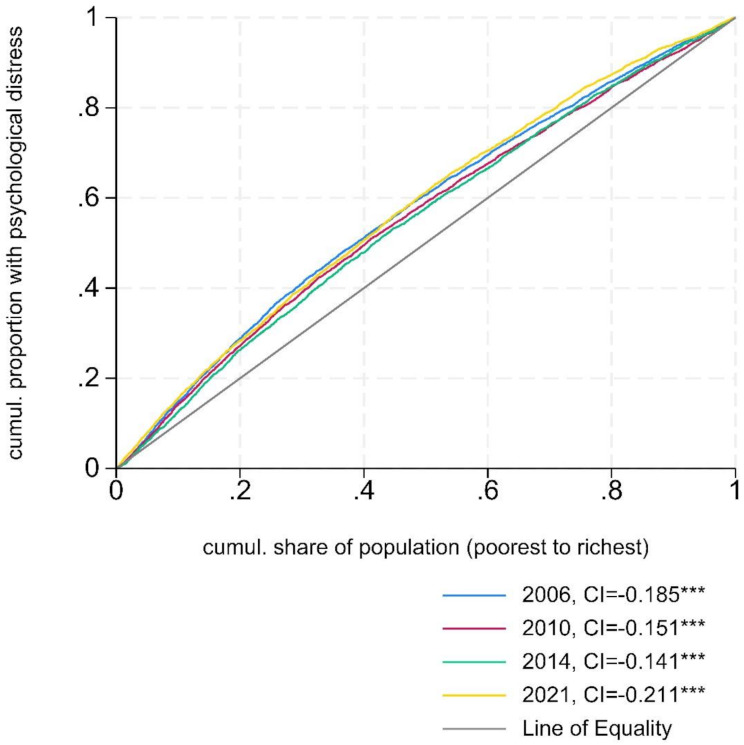
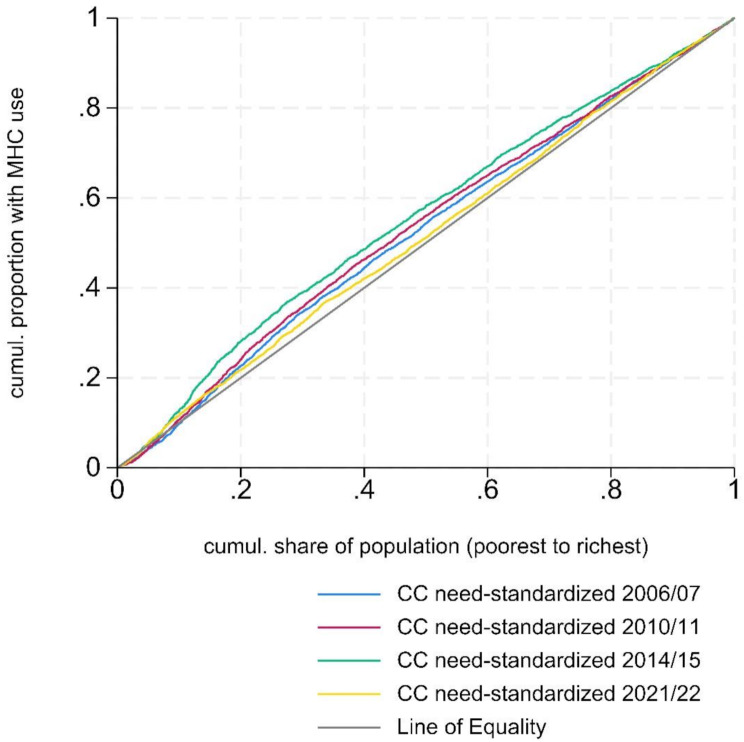
Methods: A total of 81,650 Stockholm residents aged 18-64, who participated in the Hälsa Stockholm surveys of 2006, 2010, 2014 or 2021, were analysed. Their subsequent use of MHC (primary, in- and outpatient specialized care, and psychotropic medication) within six months after survey response was collected from registries between 2006 and 2022. Concentration index (CI) and need-standardized CI (Horizontal inequity index, HI), summative measures of inequalities, were used in this study. HI was estimated using self-reported psychological distress (measured with the General health questionnaire 12 in 2006-2014 and Kessler 6 in 2021) as the primary need indicator, with general health status and long-term limiting illness as additional need indicators. Equivalized disposable household income was used as the ranking variable, while education status, migration status, age, and sex were included as non-need variables that we controlled for in the analyses.
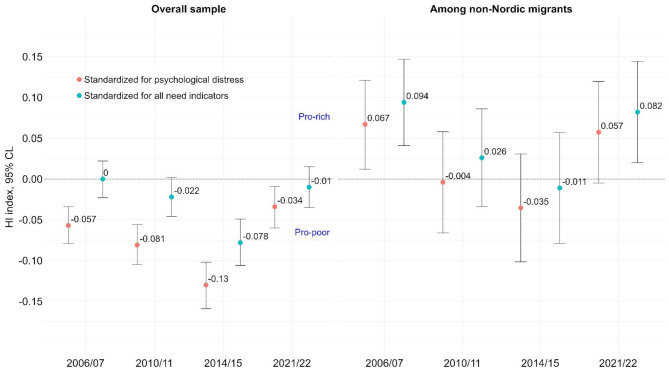
Results: Lower-income individuals used MHC services more than their higher-income counterparts with comparable levels of psychological distress. These "pro-poor" inequities in the probability of MHC use increased from HI = -0.057 [95% Confidence Limits, CL: -0.079, -0.034] in 2006/2007 to HI = -0.130 [95% CL: -0.159, -0.102] in 2014/2015. By 2021/2022, the "pro-poor" inequities had decreased (HI = -0.034 [95% CL: -0.06, -0.009]), partly due to an increase in MHC use among higher-income groups but a decrease in the lowest income group. Standardizing for additional need indicators reduced the "pro-poor" inequities but maintained the observed trends. Among non-Nordic migrants, "pro-rich" inequities fell between 2006/2007 and 2014/2015 but rose in 2021/2022, with significant "pro-rich" inequities among non-European migrants in 2021/2022 (HI = 0.100 [95% CL: 0.024, 0.176]). Among patients in outpatient services, "pro-poor" inequities in visit frequency decreased over time (2006-2022).
Conclusion: We observed increasingly higher probability of MHC use among lower-income individuals than their higher-income peers with similar (measured) needs from 2006 to 2015. However, during the pandemic (2021/2022), potential access problems led to diminishing of "pro-poor" inequities in the total sample, and to "pro-rich" inequities among non-Nordic migrants. The Covid-19 disruption to the healthcare system-such as restrictions on in-person visits and the rapid transition to digital healthcare services-along with its impact on care-seeking, may explain the trend shifts.
Keywords: Concentration index; Covid-19; Healthcare reforms; Mental disorders; Migrants.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The authors assert that this study was performed in accordance with the Helsinki Declaration of 1975, as revised in 2013. This study has ethical approval from the Swedish Ethical Review Authority (reference numbers: 2022-03050-01 & 2022-06003-02). All participants provided informed consent before participating in the Hälsa Stockholm surveys. Additional consent for the purpose of this study was waived by the Swedish Ethical Review Authority. Competing interests: All the authors except MRG and ACH are employed by Region Stockholm. Region Stockholm is responsible for all publicly-financed healthcare in Stockholm County. Consent for publication: Not applicable.
Figures
Similar articles
-
Exploring socio-economic inequalities in mental healthcare utilization in adults with self-reported psychological distress: a survey-registry linked cohort design.Epidemiol Psychiatr Sci. 2025 Jan 23;34:e6. doi: 10.1017/S2045796024000842. Epidemiol Psychiatr Sci. 2025. PMID: 39846121 Free PMC article.
-
Equitable health services for the young? A decomposition of income-related inequalities in young adults' utilization of health care in Northern Sweden.Int J Equity Health. 2017 Jan 18;16(1):20. doi: 10.1186/s12939-017-0520-3. Int J Equity Health. 2017. PMID: 28100232 Free PMC article.
-
Does the hierarchical medical system enhance healthcare utilization and equity in China? a longitudinal study 2012-2018.BMC Public Health. 2025 Aug 11;25(1):2731. doi: 10.1186/s12889-025-23933-4. BMC Public Health. 2025. PMID: 40790190 Free PMC article.
-
[Equity in Access to Health Care in Portugal: What Do We Know?].Acta Med Port. 2025 Feb 3;38(2):104-111. doi: 10.20344/amp.21668. Epub 2024 Dec 9. Acta Med Port. 2025. PMID: 39653036 Review. Portuguese.
-
Inequities to the access to and use of telemedicine among cancer patients in Europe: a scoping review.Front Public Health. 2025 May 22;13:1483706. doi: 10.3389/fpubh.2025.1483706. eCollection 2025. Front Public Health. 2025. PMID: 40475196 Free PMC article.
References
-
- Kivimäki M, Batty GD, Pentti J, Shipley MJ, Sipilä PN, Nyberg ST, et al. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: a multi-cohort study. Lancet Public Health. 2020;5(3):e140–9. - PubMed
-
- Folkhälsomyndigheten. Ojämlikheter i psykisk hälsa. Kunskapssammanställning [Inequalities in Mental Health. A review]. National Public Health Agency. 2019. Contract No.: Artikelnummer: 18122.
-
- Paananen R, Santalahti P, Merikukka M, Ramo A, Wahlbeck K, Gissler M. Socioeconomic and regional aspects in the use of specialized psychiatric care–a Finnish nationwide follow-up study. Eur J Public Health. 2013;23(3):372–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
