

A novel classification for aseptic femoral shaft nonunion after intramedullary nailing: a retrospective study
- PMID: 40200313
- PMCID: PMC11980232
- DOI: 10.1186/s12891-025-08576-1
A novel classification for aseptic femoral shaft nonunion after intramedullary nailing: a retrospective study
Abstract
Background: Although intramedullary nailing has been established as the gold standard for treating femoral shaft fractures, nonunion following intramedullary nailing remains a major concern for clinicians, severely affecting patients' walking ability and quality of life. Presently, there are certain controversies and deficiencies in nonunion classification and treatment. Herein, we propose a novel classification system for aseptic femoral shaft nonunion after intramedullary nailing based on X-ray-assessed nailing morphology and stability. Furthermore, we sought to explore the new classification's clinical significance and management implications.
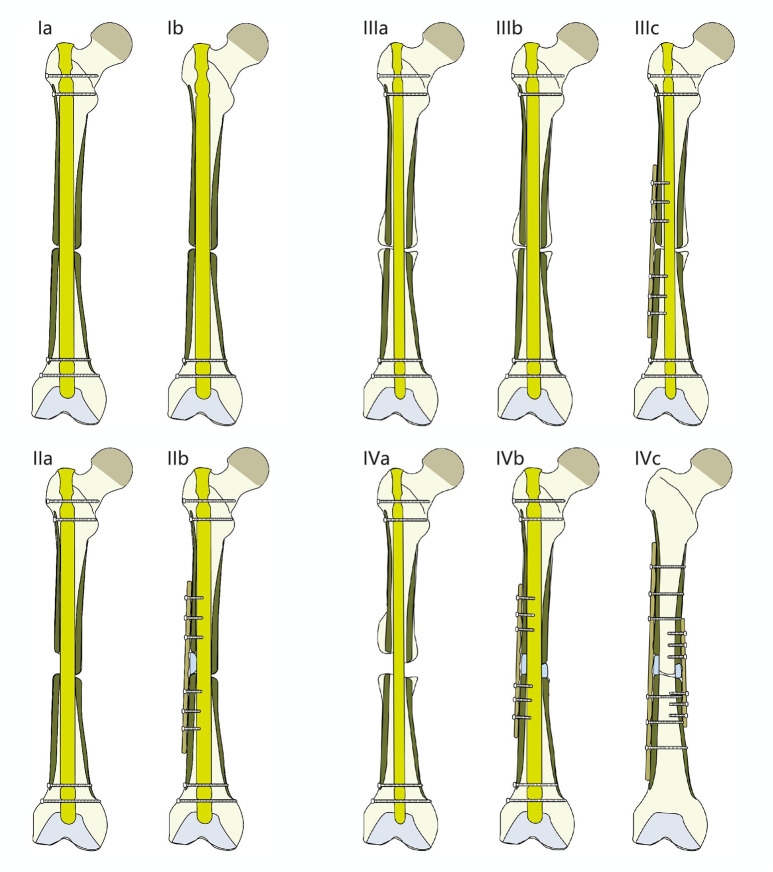
Methods: This retrospective study involved the analysis of clinical data collected from 82 patients with aseptic bone nonunion after intramedullary nailing of femoral shaft fractures between 2010 and 2022. The patients were classified into four groups based on intramedullary nailing stability and bone defect existence, as revealed in X-ray images. The four classifications were as follows: Type I (intramedullary nailing is stable without bone defect), Type II (intramedullary nailing is stable with bone defect), Type III (intramedullary nailing is not stable without bone defect), and Type IV (intramedullary nailing is not stable with bone defect). Based on the novel classifications, we introduced individualized treatment methods. Type I patients underwent dynamization, and Type II patients received bone grafting and plate fixation. Type III patients underwent larger intramedullary nail exchange or plate fixation, and Type IV patients received larger intramedullary nail exchange and plate fixation with bone graft or double plate fixation with bone graft. Data on relevant indicators were collected.
Results: All patients recovered well with no complications. The average surgery times for Types I-IV were 0.4 ± 0.1, 0.8 ± 0.2, 1.1 ± 0.4, and 1.6 ± 0.4 h, respectively. Furthermore, the mean blood loss volumes for Types I-IV were 23.4 ± 4.8, 53.3 ± 8.4, 56.3 ± 7.9, and 125.2 ± 10.8 ml, respectively. The average bone healing time of all 82 patients was 5.1 ± 1.5 months. On the other hand, the mean bone healing times for Types I-IV were 4.6 ± 1.1, 4.7 ± 1.1, 5.1 ± 1.5, and 5.7 ± 1.8 months, respectively. Furthermore, the LEFS scores for Types I-IV were 68.7 ± 3.5, 69.8 ± 3.1, 66.8 ± 3.8, and 68.6 ± 2.9 points, respectively. The mean surgery time and bleeding volume increased gradually from Types I to IV (p < 0.05) but with no significant difference between Types II and III. Moreover, there were no statistical differences in fracture healing times, LEFS scores, age, and nonunion durations across the four classifications.
Conclusions: The proposed novel classification system could achieve accurate diagnosis and guidance for clinical management of aseptic femoral shaft nonunion after intramedullary nailing. The corresponding individualized treatment approaches could improve prognostic outcomes and healing rates and alleviate postoperative complications.
Clinical trial number: Not applicable.
Keywords: Aseptic femoral shaft nonunion; Femoral shaft fracture; Intramedullary nailing; Nonunion classification.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Approval was obtained from the Ethical Committee of Shanghai Baoshan Luodian Hospital. Informed consent was obtained from all individual patients included in the study. Consent for publication: All participants were informed about publication. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Aseptic femoral nonunion treated with exchange locked nailing with intramedullary augmentation cancellous bone graft.J Orthop Surg Res. 2022 Jul 6;17(1):339. doi: 10.1186/s13018-022-03229-8. J Orthop Surg Res. 2022. PMID: 35794570 Free PMC article.
-
Comparing outcomes of plate augmentation, nail exchange, and nail exchange with plate augmentation in the treatment of atrophic femoral shaft nonunion after intramedullary nailing: a multicenter retrospective study.Arch Orthop Trauma Surg. 2024 Mar;144(3):1259-1268. doi: 10.1007/s00402-023-05183-4. Epub 2024 Feb 19. Arch Orthop Trauma Surg. 2024. PMID: 38372763
-
Augmentation plating leaving the nail in situ is an excellent option for treating femoral shaft nonunion after IM nailing: a multicentre study.Eur J Trauma Emerg Surg. 2021 Dec;47(6):1895-1901. doi: 10.1007/s00068-020-01333-0. Epub 2020 Feb 27. Eur J Trauma Emerg Surg. 2021. PMID: 32107562
-
[Recent advances in treatment of aseptic femoral shaft nonunion].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018 May 15;32(5):519-525. doi: 10.7507/1002-1892.201712089. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018. PMID: 29806336 Free PMC article. Review. Chinese.
-
Diagnostic and treatment modalities in nonunions of the femoral shaft: a review.Injury. 2012 Jul;43(7):980-8. doi: 10.1016/j.injury.2011.06.030. Epub 2011 Jul 8. Injury. 2012. PMID: 21741650 Review.
References
-
- Song W, Xu WZ, Liu H, Luo DQ, Zhang JH, Wu J. [A comparative study of postoperative efficacy between antegrade and retrograde intramedullary nailing in the treatment of middle femoral shaft fractures]. J Practical Orthop. 2024;30(1):24–8.
-
- Lai PJ, Hsu YH, Chou YC, Yeh WL, Ueng SWN, Yu YH. Augmentative antirotational plating provided a significantly higher union rate than exchanging reamed nailing in treatment for femoral shaft aseptic atrophic nonunion - retrospective cohort study. BMC Musculoskelet Disord. 2019;20(1):127. - PMC - PubMed
-
- Pihlajamäki HK, Salminen ST, Böstman OM. The treatment of nonunions following intramedullary nailing of femoral shaft fractures. J Orthop Trauma. 2022;16(6):394–402. - PubMed
-
- Weber BG, Čech O. Pseudarthrosis: pathophysiology, biomechanics, therapy, results. Grune & Stratton; 1976.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
