

Bacterial infection in patients with juvenile systemic lupus erythematosus and fever
- PMID: 40200360
- PMCID: PMC11980166
- DOI: 10.1186/s12969-025-01088-1
Bacterial infection in patients with juvenile systemic lupus erythematosus and fever
Abstract
Background: Juvenile Systemic Lupus Erythematosus (JSLE) is a chronic, systemic autoimmune disease characterized by an increased susceptibility to infections. Fever in these patients can result from infection, heightened lupus activity, or a combination of both. Various clinical factors and biomarkers have been proposed to differentiate between infection and disease activity, but the results remain inconclusive. The Systemic Lupus Erythematosus Disease Activity Index-2000 (SLEDAI-2 k) is used to assess lupus activity in the presence or absence of infection. This study aimed to identify factors associated with bacterial infections in JSLE patients presenting with fever.
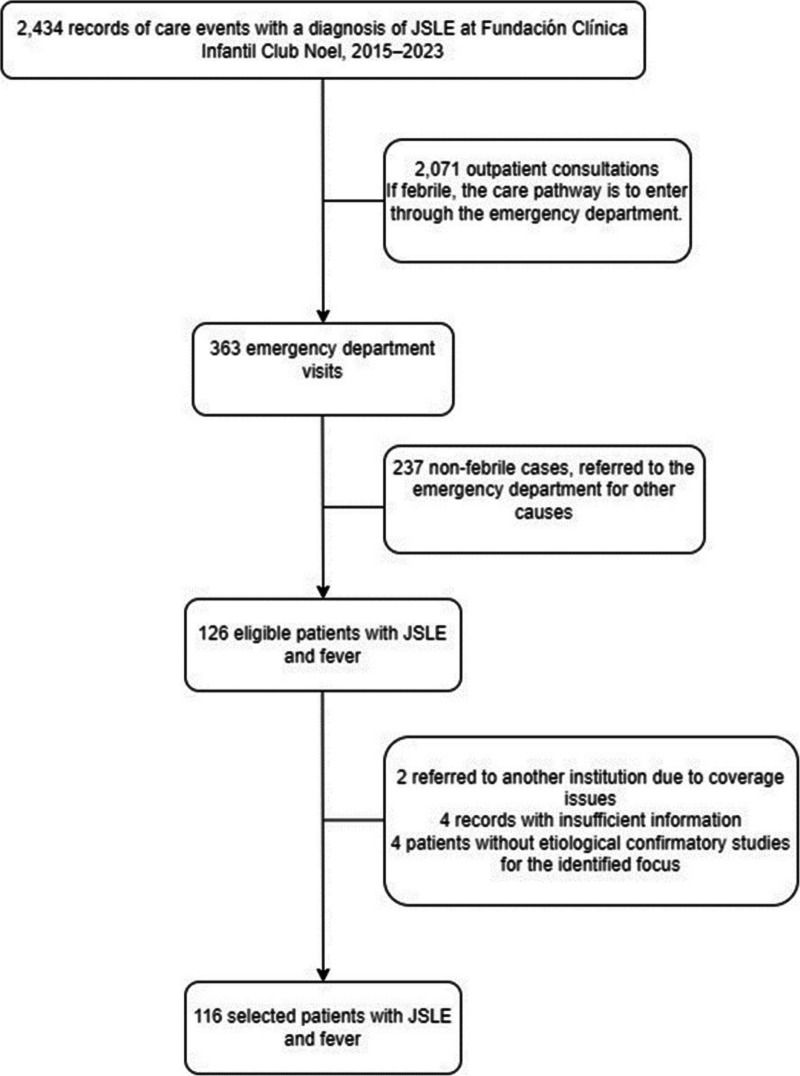
Methods: A case-control study, approved by the institutional ethics committee, was conducted.
Results: Bacterial infection was identified in 17% of 116 patients. Factors evaluated included immunomodulator use, high-dose steroids, renal replacement therapy, erythrocyte sedimentation rate (ESR) > 20, C-reactive protein (CRP) > 60 and > 90 mg/L, ferritin > 500 ng/mL, neutrophil-to-lymphocyte ratio (NLR) > 6, platelet-to-lymphocyte ratio (PLR) > 133, procalcitonin (PCT) > 0.9 ng/mL, lymphocyte-to-C4 ratio (LC4R) > 66.7, and ESR/CRP ratio < 2. In the adjusted model, PCT > 0.9 ng/mL retained significance with p < 0.01. Nagelkerke's R2 was 0.65, and the Hosmer-Lemeshow test indicated good internal validity.
Conclusions: Bacterial infection was detected in 17% of JSLE patients with fever. Procalcitonin > 0.9 ng/mL is a critical marker for identifying bacterial infection. NLR, PLR, ESR/CRP ratio, LC4R, and ferritin require further investigation to establish definitive cut-off values for differentiating bacterial infections from other infections or disease activity. Individual patient evaluation remains the recommended approach for diagnosis.
Keywords: Bacteria; Biomarkers; Fever; Systemic lupus erythematosus.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Approved by Fundación Clínica Infantil Club Noel Ethical Committee for Research, and Bioethical and Ethical Committee for Research at Universidad Libre, Sectional Cali. Consent for publication: Not applied for this study. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Infection versus disease activity in systemic lupus erythematosus patients with fever.BMC Rheumatol. 2024 Aug 14;8(1):34. doi: 10.1186/s41927-024-00395-6. BMC Rheumatol. 2024. PMID: 39143483 Free PMC article.
-
The use of procalcitonin determinations in evaluation of systemic lupus erythematosus.J Clin Rheumatol. 2008 Jun;14(3):138-42. doi: 10.1097/RHU.0b013e3181772cca. J Clin Rheumatol. 2008. PMID: 18525431
-
Serum procalcitonin and C-reactive protein for differentiating bacterial infection from disease activity in patients with systemic lupus erythematosus.Mod Rheumatol. 2014 May;24(3):457-63. doi: 10.3109/14397595.2013.844391. Epub 2013 Oct 21. Mod Rheumatol. 2014. PMID: 24252006
-
Serum procalcitonin and C-reactive protein levels as diagnostic markers for distinguishing bacterial infections from lupus flares in systemic lupus erythematosus: A systematic review and meta‑analysis.Int Immunopharmacol. 2021 Dec;101(Pt B):108304. doi: 10.1016/j.intimp.2021.108304. Epub 2021 Oct 30. Int Immunopharmacol. 2021. PMID: 34731783
-
Platelet-to-lymphocyte ratio as a biomarker of systemic inflammation in systemic lupus erythematosus: A meta-analysis and systematic review.PLoS One. 2024 May 16;19(5):e0303665. doi: 10.1371/journal.pone.0303665. eCollection 2024. PLoS One. 2024. PMID: 38753735 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
