

Pulmonary Tumor Thrombotic Microangiopathy Associated With Gastric Cancer: Clinical Characteristics and Outcomes
- PMID: 40200872
- PMCID: PMC11982500
- DOI: 10.5230/jgc.2025.25.e1
Pulmonary Tumor Thrombotic Microangiopathy Associated With Gastric Cancer: Clinical Characteristics and Outcomes
Abstract
Purpose: Pulmonary tumor thrombotic microangiopathy (PTTM) is a fatal complication of gastric cancer (GC). This study aimed to evaluate the clinical characteristics, outcomes, and immunohistochemical profiles of patients with GC-induced PTTM.
Materials and methods: From 2011 to 2023, 8 patients were clinically diagnosed with PTTM associated with GC antemortem. Clinical features and outcomes were reviewed, and immunohistochemical staining for c-erbB-2, MutL protein homolog 1, and programmed cell death ligand-1 was performed.
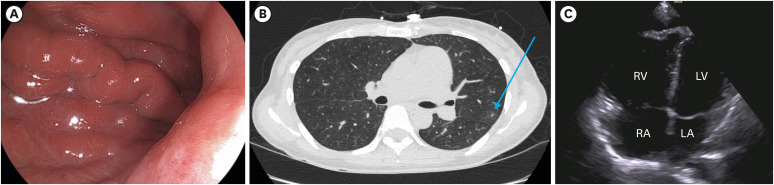
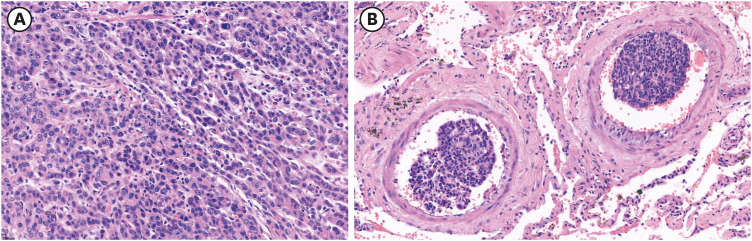
Results: The median patient age was 56 years (range, 34-66 years). In all the patients, the tumors exhibited either ulceroinfiltrative or diffusely infiltrative gross morphology. The median tumor size was 5.8 cm (range, 2.0 cm-15.0 cm). Poorly differentiated adenocarcinoma was the most common histological type (6/8, 75%), followed by signet ring cell carcinoma (1/8, 12.5%) and moderately differentiated adenocarcinoma (1/8, 12.5%). Chest computed tomography revealed ground-glass opacities (7/8, 87.5%) or tree-in-bud signs (2/8, 25.0%) without definite evidence of pulmonary thromboembolism. Disseminated intravascular coagulation was present in 62.5% (5/8) of the patients diagnosed with PTTM. C-erbB-2 was positive in one patient (1/8, 12.5%). One patient who received palliative chemotherapy after developing PTTM survived for 35 days, whereas the other 7 patients who did not receive chemotherapy after developing PTTM survived for 7 days or less after PTTM diagnosis.
Conclusions: Most patients with GC-induced PTTM had an undifferentiated-type histology, infiltrative morphology, and extremely poor survival. Palliative chemotherapy may benefit patients with GC-induced PTTM; however, further studies are needed to explore the potential of targeted therapy in these patients.
Keywords: Gastric cancer; Prognosis; Pulmonary tumor thrombotic microangiopathy.
Copyright © 2025. Korean Gastric Cancer Association.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- von Herbay A, Illes A, Waldherr R, Otto HF. Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension. Cancer. 1990;66:587–592. - PubMed
-
- Chinen K, Tokuda Y, Fujiwara M, Fujioka Y. Pulmonary tumor thrombotic microangiopathy in patients with gastric carcinoma: an analysis of 6 autopsy cases and review of the literature. Pathol Res Pract. 2010;206:682–689. - PubMed
-
- Uruga H, Fujii T, Kurosaki A, Hanada S, Takaya H, Miyamoto A, et al. Pulmonary tumor thrombotic microangiopathy: a clinical analysis of 30 autopsy cases. Intern Med. 2013;52:1317–1323. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
