

Efficacy and safety of Jinghua Weikang capsule combined with amoxicillin-furazolidone triple/quadruple therapies in the rescue treatment of Helicobacter pylori infection
- PMID: 40201322
- PMCID: PMC11975852
- DOI: 10.3389/fmed.2025.1531620
Efficacy and safety of Jinghua Weikang capsule combined with amoxicillin-furazolidone triple/quadruple therapies in the rescue treatment of Helicobacter pylori infection
Abstract
Aim: To evaluate the efficacy and safety of Jinghua Weikang Capsule (JWC) combined with amoxicillin-furazolidone triple/quadruple therapies in the rescue treatment of drug-resistant H. pylori infection.
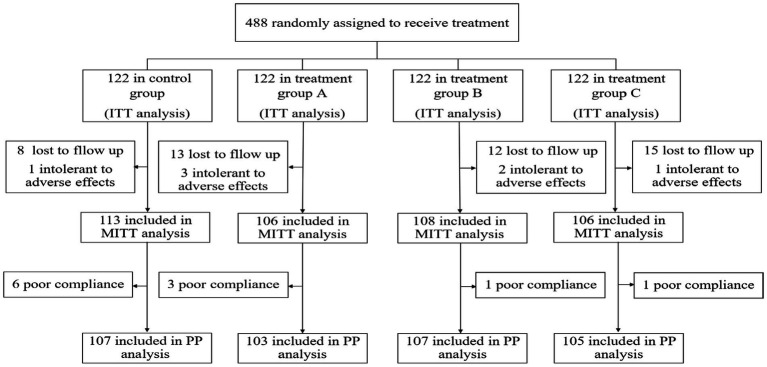
Methods: Patients who failed H. pylori eradication therapy at least once were enrolled and randomly assigned into four groups (1:1:1:1), as follows: The control group received 20 mg rabeprazole, 1,000 mg amoxicillin, 220 mg bismuth potassium citrate, and 100 mg furazolidone twice daily (b.i.d.) for 14 days; Group A received 240 mg JWC b.i.d. combined with 20 mg rabeprazole, 1,000 mg amoxicillin, and 100 mg furazolidone b.i.d. for 14 days; Group B received the same regimen as Group A for 14 days, followed by an additional 14 days of 240 mg JWC b.i.d.; and Group C received 240 mg JWC b.i.d. combined with 20 mg rabeprazole, 1,000 mg amoxicillin, 220 mg bismuth potassium citrate, and 100 mg furazolidone b.i.d. for 10 days. The primary outcome was H. pylori eradication at 4 weeks after treatment.
Results: Four hundred eighty-eight patients were included in this study. The intention-to-treat (ITT) eradication rates in the four groups were 85.2, 73.8, 78.7 and 75.4% (p = 0.136), while the modified intention-to-treat (MITT) eradication rates were 92.0, 84.9, 88.9 and 86.8% (p = 0.398), respectively. And the per-protocol (PP) eradication rates were 92.5, 85.4, 87.9 and 86.7% (p = 0.405), respectively. The eradication rates were comparable among the four groups. No statistically significant differences in eradication rates were observed between each of the three treatment groups and the control group (all p > 0.05). The eradication rate of H. pylori in group B demonstrated non-inferiority compared with the control group (p = 0.0415; 90% CI, -0.0965 to 0.0336). The four groups exhibited similar frequencies of overall adverse events (9.84, 5.74, 6.56%, 2.46%, p = 0.112).
Conclusion: The eradication rate of the JWC-containing regimen demonstrated no statistically significant difference compared with bismuth-containing quadruple therapy in the rescue treatment of H. pylori infection. The prolonged JWC treatment regimen exhibited non-inferiority in eradication rates. JWC-containing therapies can effectively reduce the incidence of adverse reactions and significantly alleviate certain clinical symptoms.
Clinical trial: https://clinicaltrials.gov/, identifier ChiCTR1800019326.
Keywords: Helicobacter pylori; Jinghua Weikang capsule; bismuth-containing quadruple therapy; multi-center randomized controlled study; rescue treatment.
Copyright © 2025 Yang, Deng, Xiao, Ye, Wang, Jiang, Han, Wang, Ma, Lan, Ye and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Similar articles
-
Efficacy and safety of high-dose esomeprazole-amoxicillin dual therapy for Helicobacter pylori rescue treatment: a multicenter, prospective, randomized, controlled trial.Chin Med J (Engl). 2022 Jul 20;135(14):1707-1715. doi: 10.1097/CM9.0000000000002289. Chin Med J (Engl). 2022. PMID: 36193978 Free PMC article. Clinical Trial.
-
[Jinghuaweikang capsules combined with furazolidone-based triple or quadruple therapy as the rescue treatment for Helicobacter pylori infection: a multicenter randomized controlled clinical trial].Zhonghua Yi Xue Za Zhi. 2016 Nov 1;96(40):3206-3212. doi: 10.3760/cma.j.issn.0376-2491.2016.40.002. Zhonghua Yi Xue Za Zhi. 2016. PMID: 27852385 Clinical Trial. Chinese.
-
Furazolidone-based triple and quadruple eradication therapy for Helicobacter pylori infection.World J Gastroenterol. 2014 Aug 28;20(32):11415-21. doi: 10.3748/wjg.v20.i32.11415. World J Gastroenterol. 2014. PMID: 25170230 Free PMC article. Clinical Trial.
-
Jinghua Weikang capsule for helicobacter pylori eradication: A systematic review and meta-analysis with trial sequential analysis.Front Pharmacol. 2022 Sep 26;13:959184. doi: 10.3389/fphar.2022.959184. eCollection 2022. Front Pharmacol. 2022. PMID: 36225593 Free PMC article.
-
Second-line rescue treatment of Helicobacter pylori infection: Where are we now?World J Gastroenterol. 2018 Oct 28;24(40):4548-4553. doi: 10.3748/wjg.v24.i40.4548. World J Gastroenterol. 2018. PMID: 30386104 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous