

Bilateral Adrenal Nodules in the Setting of Disseminated Fungal Infection: An Important Consideration for Appropriate Management of Adrenal Pathology
- PMID: 40201468
- PMCID: PMC11973672
- DOI: 10.1016/j.aace.2024.12.003
Bilateral Adrenal Nodules in the Setting of Disseminated Fungal Infection: An Important Consideration for Appropriate Management of Adrenal Pathology
Abstract
Background/objective: Increased utilization of cross-sectional imaging has led to a rise in diagnosis of incidental adrenal lesions. Physicians in many clinical settings are increasingly faced with addressing these incidental lesions by initiating the correct workup, diagnosis, and long-term follow-up plan. Our objective was to demonstrate the importance of maintaining a broad differential and completing a thorough workup in determining the correct treatment plan for patients with bilateral adrenal lesions.
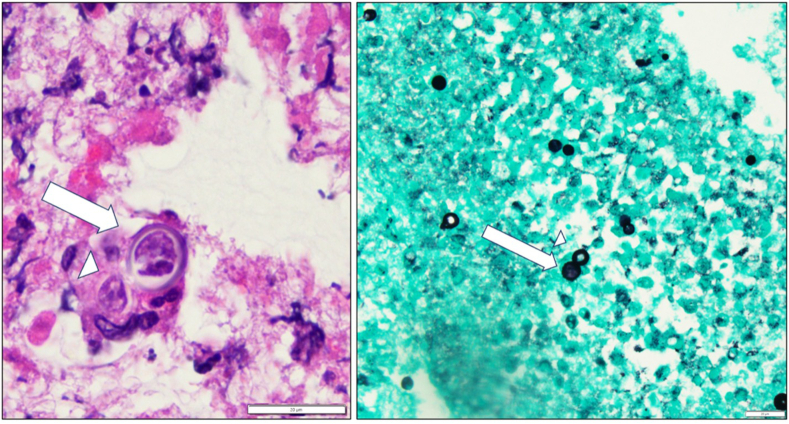
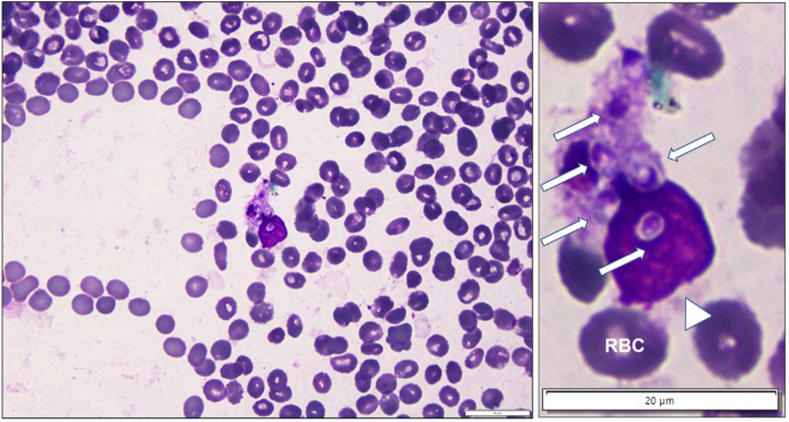
Case report: We present 2 patients who recently completed chemotherapy for lymphoma, found to have new bilateral adrenal lesions on postchemotherapy imaging. Urine antigen and/or adrenal biopsy was performed to confirm the diagnosis of disseminated fungal infection. This diagnosis has major implications on the treatment plan, which includes antifungal therapy instead of surgical management or additional chemotherapy. Cross-sectional imaging after initiation of antifungal treatment demonstrated decreasing size of nodules.
Discussion: A broad differential is critical when working up and developing treatment plans for adrenal nodules, specifically considering a fungal etiology in the setting of immunosuppression or primary extra-adrenal malignancy.
Conclusion: Incidentally found adrenal lesions are becoming more common, and in turn, the obligation for appropriate management of adrenal pathology not only falls to medical and surgical endocrinologists but also to general practitioners. It is prudent to consider atypical etiologies including disseminated fungal infection prior to surgical excision or initiation of chemotherapy as those treatment strategies would not benefit select patients.
Keywords: adrenal mycosis; bilateral adrenal nodules; blastomycosis; histoplasmosis; incidentaloma.
© 2025 AACE. Published by Elsevier Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources