

Bridging radiotherapy before chimeric antigen receptor T cells for B-cell lymphomas: an ILROG multicenter study
- PMID: 40203192
- PMCID: PMC12268022
- DOI: 10.1182/bloodadvances.2025015855
Bridging radiotherapy before chimeric antigen receptor T cells for B-cell lymphomas: an ILROG multicenter study
Abstract
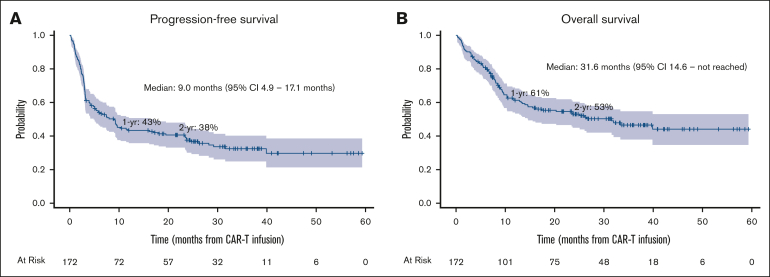
Despite the increasing utilization of bridging radiotherapy (Br-RT), its impact on chimeric antigen receptor T-cell therapy (CAR-T) efficacy and toxicity remains poorly characterized. We retrospectively reviewed patients with relapsed/refractory B-cell lymphomas (BCLs) who received Br-RT followed by CAR-T from 2018 to 2020 across 10 institutions. Br-RT toxicities were graded per Common Terminology Criteria for Adverse Events version 5.0, and cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) per American Society for Transplantation and Cellular Therapy Consensus Guidelines. One hundred seventy-two patients (168 large BCL) received Br-RT before axicabtagene ciloleucel (73%), tisagenlecleucel (24%), or brexucabtagene autoleucel (2%). At leukapheresis, most patients (74%) had advanced-stage disease and 39% had bulky disease measuring ≥10cm. Comprehensive Br-RT was administered to 39% and bridging systemic therapy to 35%. Among all patients, grade ≥3 Br-RT toxicity occurred in 2% (1 grade 5 toxicity), grade ≥3 CRS in 9%, and grade ≥3 ICANS in 24%. Median follow-up was 31.3 months. Two-year progression-free survival (PFS) and overall survival (OS) were 38% and 53%, respectively. On multivariable analysis, comprehensive Br-RT was associated with superior PFS (hazard ratio [HR], 0.38; P < .001) and OS (HR, 0.48; P = .011). Patients with lactate dehydrogenase (LDH) normalization after Br-RT (high pre-Br-RT LDH, normal post-Br-RT LDH) had superior PFS and OS compared with those with high post-Br-RT LDH and similar PFS and OS compared with those with normal baseline LDH. In this particularly high-risk cohort, Br-RT before CAR-T demonstrates an acceptable toxicity profile with favorable clinical outcomes compared with historical controls. Comprehensive Br-RT and LDH normalization after Br-RT may be associated with superior PFS and OS.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: E.A.C. reports research funding from Genmab, AbbVie, AstraZeneca, CARGO, Genentech/Roche, and Nurix, and has consulted for AstraZeneca, BeiGene, Genmab, and AbbVie. N.M.D. reports research funding from Bristol Myers Squibb and serves on the advisory board for Miltenyi Biotec. S.J.S. reports research funding from Genentech/Roche, Genmab, and Nurix; has consulted for AbbVie, AstraZeneca, BeiGene, BioNTech, Genentech, Genmab, Janssen, Kite Pharmaceuticals, Legend Biotech, MorphoSys, and Novartis; and serves on steering committees for Caribou Biosciences and Novartis. P.M.R. reports research funding from Genentech and Seagen; has consulted for Caribou Biosciences and Kite Gilead; and has received speaking fees from Kite Gilead. M.J.D. reports research funding from Kite Gilead, Incyte, and Eli Lilly, and has consulted for and provides advisory to Kite Gilead and Novartis. The remaining authors declare no competing financial interests.
Figures





References
-
- Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396(10254):839–852. - PubMed
-
- Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. 2019;380(1):45–56. - PubMed
-
- Saifi O, Breen WG, Lester SC, et al. Does bridging radiation therapy affect the pattern of failure after CAR T-cell therapy in non-Hodgkin lymphoma? Radiother Oncol. 2022;166:171–179. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
