

Psilocybin therapy for mood dysfunction in Parkinson's disease: an open-label pilot trial
- PMID: 40205013
- PMCID: PMC12170852
- DOI: 10.1038/s41386-025-02097-0
Psilocybin therapy for mood dysfunction in Parkinson's disease: an open-label pilot trial
Abstract
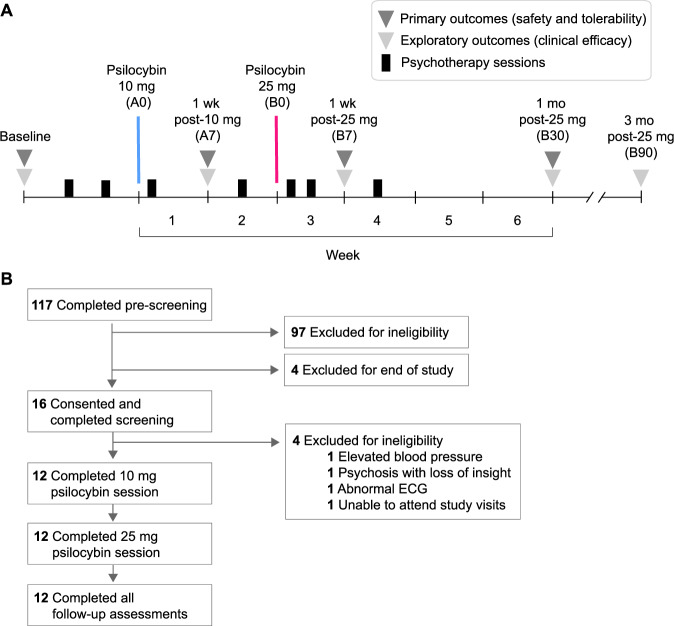
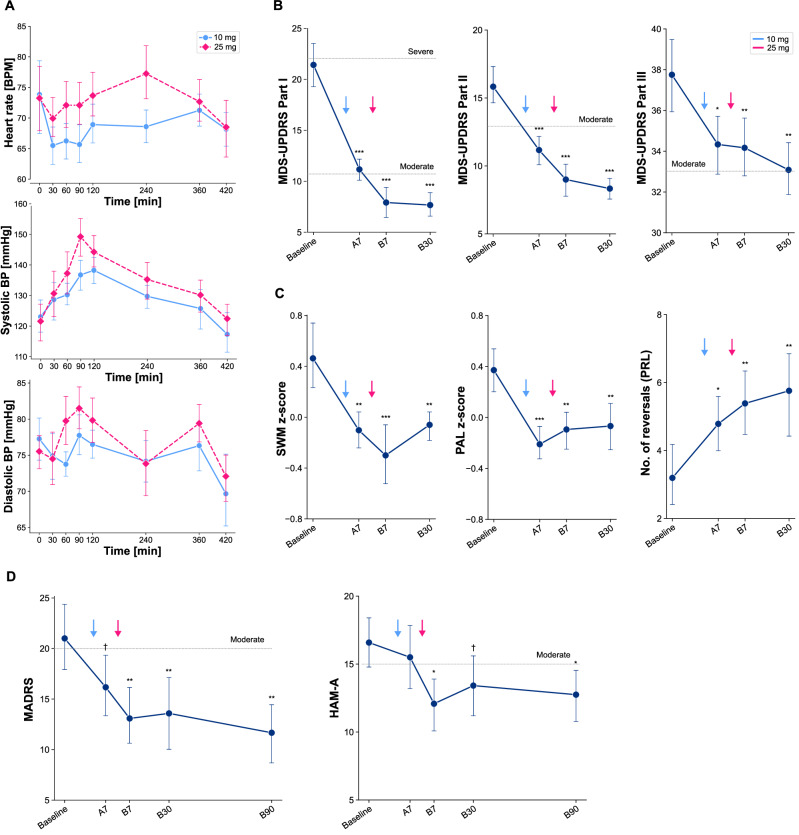
Mood dysfunction is highly prevalent in Parkinson's disease (PD), a main predictor of functional decline, and difficult to treat-novel interventions are critically needed. Psilocybin shows early promise for treating depression and anxiety, but its potential in PD is unknown, as safety concerns have excluded people with neurodegenerative disease from previous trials. In this open-label pilot (NCT04932434), we examined the feasibility of psilocybin therapy among people with mild to moderate stage PD plus depression and/or anxiety. 12 participants (mean age 63.2 ± 8.2 years, 5 women) received psilocybin (one 10 mg followed by one 25 mg dose) with psychotherapy. There were no serious adverse events, no medical interventions required to manage effects of psilocybin, and no exacerbation of psychosis. Ten participants experienced treatment-emergent adverse events; the most frequent were anxiety, nausea, and increased blood pressure. We observed no worsening of PD symptomology measured by the Movement Disorder Society Unified Parkinson's Disease Rating Scale (MDS-UPDRS). On the contrary, non-motor (MDS-UPDRS Part I: -13.8 ± 1.3, p < 0.001, Hedges' g = 3.0) and motor symptoms (Part II: -7.5 ± 0.9, p < 0.001, g = 1.2; Part III: -4.6 ± 1.3, p = 0.001; g = 0.3) as well as performance in select cognitive domains (Paired Associates Learning [-0.44 ± 0.14, p = .003, g = 0.4], Spatial Working Memory [-0.52 ± 0.17, p = 0.003, g = 0.7], and Probabilistic Reversal Learning [2.9 ± 0.9, p = 0.003, g = 1.3]) improved post-treatment, and improvements were sustained until the final safety assessment one month following drug exposure. Baseline Montgomery-Asberg Depression Rating Scale (MADRS) and Hamilton Anxiety Rating Scale (HAM-A) scores were 21.0 ± 8.7 and 17.0 ± 3.7, respectively. Both improved to a clinically meaningful degree post-treatment; these improvements persisted to the final assessment three months following drug exposure (MADRS: -9.3 ± 2.7, p = .001, g = 1.0; HAM-A: -3.8 ± 1.7; p = 0.031, g = 0.7). This study provides the first data on psilocybin's effects in any neurodegenerative disease. Results suggest that psilocybin therapy in PD warrants further investigation.
© 2025. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Competing interests: AO has received research support from SILO Inc. and Filament Health. ADP has received research support from the Multidisciplinary Association for Psychedelic Studies (MAPS), Usona Institute, and Filament Health. He has consulted for Tactogen, Osmind, Compass Pathways, Mindmed, and Alexander Shulgin Research Institute. He has served on the advisory boards of Otsuka, Alkermes. He is a shareholder in Tactogen and Osmind. JDW has received research support from Usona Institute and Filament Health. He has consulted for Alexander Shulgin Research Institute, Guidepoint, Magdalena Biosciences, Arcadia Medicine, MindMed, and Techspert.IO. The other authors declare no competing interests.
Figures
References
-
- Jellinger KA. Neuropathology of nonmotor symptoms of Parkinson’s disease. Int. Rev. Neurobiol., vol. 133, Elsevier; 2017. p. 13–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
