

Monitoring patients with acute respiratory failure during non-invasive respiratory support to minimize harm and identify treatment failure
- PMID: 40205493
- PMCID: PMC11983977
- DOI: 10.1186/s13054-025-05369-9
Monitoring patients with acute respiratory failure during non-invasive respiratory support to minimize harm and identify treatment failure
Abstract
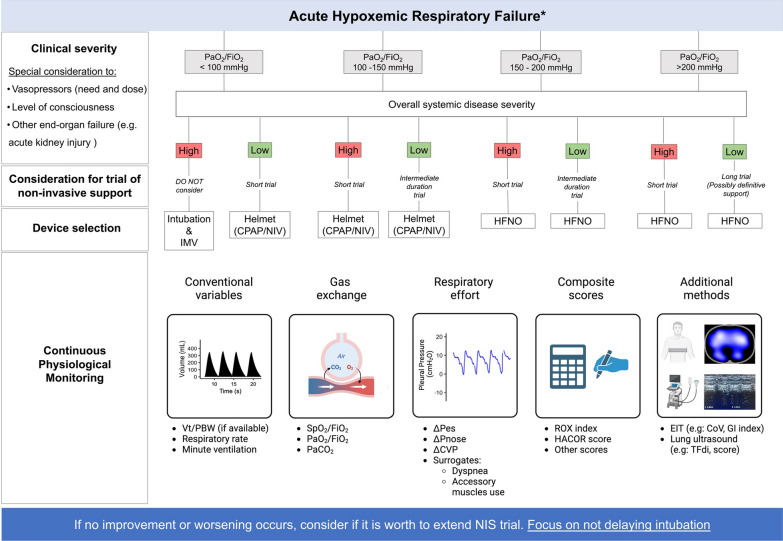
Non-invasive respiratory support (NRS), including high flow nasal oxygen therapy, continuous positive airway pressure and non-invasive ventilation, is a cornerstone in the management of critically ill patients who develop acute respiratory failure (ARF). Overall, NRS reduces the work of breathing and relieves dyspnea in many patients with ARF, sometimes avoiding the need for intubation and invasive mechanical ventilation with variable efficacy across diverse clinical scenarios. Nonetheless, prolonged exposure to NRS in the presence of sustained high respiratory drive and effort can result in respiratory muscle fatigue, cardiovascular collapse, and impaired oxygen delivery to vital organs, leading to poor outcomes in patients who ultimately fail NRS and require intubation. Assessment of patients' baseline characteristics before starting NRS, close physiological monitoring to evaluate patients' response to respiratory support, adjustment of device settings and interface, and, most importantly, early identification of failure or of paramount importance to avoid the negative consequences of delayed intubation. This review highlights the role of respiratory monitoring across various modalities of NRS in patients with ARF including dyspnea, general respiratory parameters, measures of drive and effort, and lung imaging. It includes technical specificities related to the target population and emphasizes the importance of clinicians' physiological understanding and tailoring clinical decisions to individual patients' needs.
Keywords: Acute respiratory failure; Non-invasive respiratory support; Respiratory monitoring.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: IT reports personal fees from Medtronic and MbMed SA not related to the current work.
Figures
Similar articles
-
Non-invasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ARDS.Intensive Care Med. 2021 Aug;47(8):851-866. doi: 10.1007/s00134-021-06459-2. Epub 2021 Jul 7. Intensive Care Med. 2021. PMID: 34232336 Free PMC article. Review.
-
Monitoring and modulation of respiratory drive in patients with acute hypoxemic respiratory failure in spontaneous breathing.Intern Emerg Med. 2024 Nov;19(8):2105-2119. doi: 10.1007/s11739-024-03715-3. Epub 2024 Aug 29. Intern Emerg Med. 2024. PMID: 39207721 Free PMC article. Review.
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial.JAMA. 2021 May 4;325(17):1731-1743. doi: 10.1001/jama.2021.4682. JAMA. 2021. PMID: 33764378 Free PMC article. Clinical Trial.
-
Effect of non-invasive oxygenation strategies in immunocompromised patients with severe acute respiratory failure: a post-hoc analysis of a randomised trial.Lancet Respir Med. 2016 Aug;4(8):646-652. doi: 10.1016/S2213-2600(16)30093-5. Epub 2016 May 27. Lancet Respir Med. 2016. PMID: 27245914 Clinical Trial.
References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA J Am Med Assoc. 2016;315:788–800. - PubMed
-
- Levy MM. Pathophysiology of oxygen delivery in respiratory failure. Chest. 2005;128:547S-553S. - PubMed
-
- Lorente JA, Renes E, Gómez-Aguinaga MA, Landín L, de la Morena JL, Liste D. Oxygen delivery-dependent oxygen consumption in acute respiratory failure. Crit Care Med. 1991;19:770–5. - PubMed
-
- Vieira F, Bezerra FS, Coudroy R, Schreiber A, Telias I, Dubo S, et al. High-flow nasal cannula compared with continuous positive airway pressure: a bench and physiological study. J Appl Physiol. 2022;132:1580–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
