Gastric Myoelectrical Activity Subtypes in Functional Dyspepsia and Gastroparesis
- PMID: 40205899
- PMCID: PMC11986652
- DOI: 10.5056/jnm24049
Gastric Myoelectrical Activity Subtypes in Functional Dyspepsia and Gastroparesis
Abstract
Background/aims: Gastric dysrhythmias, loss of normal 3 cycles per minute (CPM) gastric myoelectrical activity (GMA), and variable loss of interstitial cells of Cajal are reported both in gastroparesis (GP) and functional dyspepsia (FD). We hypothesize that the patients with GP, and FD with normal gastric emptying (NGE) and delayed gastric emptying (DGE) may vary in symptom severity, and GMA profiles.
Methods: Symptoms and their severity were evaluated by gastroparesis cardinal symptom index (GCSI), Abell scoring, short-form Nepean dyspepsia index (SF-NDI), the World Health Organization quality of life, and Rome IV subtyping for FD. Solid-meal gastric emptying was assessed by nuclear scintigraphy. Water load satiety test (WLST)-based electrogastrography determined GMA.
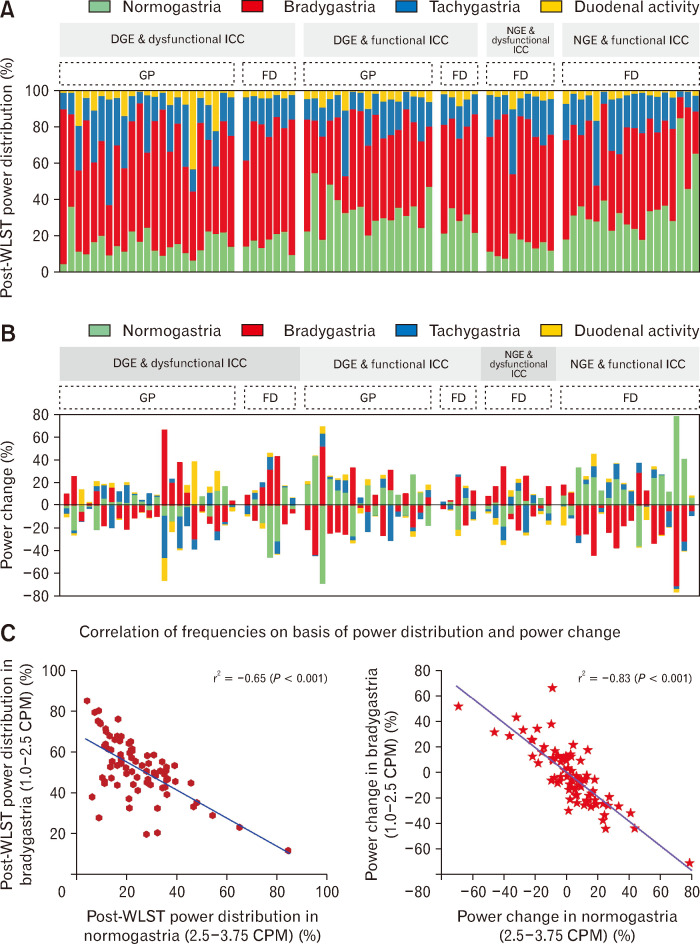
Results: Patients with GP (n = 40) had higher GCSI than those with FD (n = 39; [12 DGE, 27 NGE] (2.79 [2.17-3.33] vs 1.67 [0.83-2.61] vs 0.83 [0.55-1.93]; P < 0.001, in GP vs FD-NGE vs FD-DGE, respectively), severe Abell grade (Grade III in 17 [43%] vs 0% vs 0%, in GP vs FD-NGE vs FD-DGE, respectively), severe SF-NDI (80.5 [63.5-102.5] vs 50 [27-91] vs 30 [21.25-45.5]); and poor QOL. Sixteen (40%) GP had impaired gastric accommodation (< 238 mL). Post-WLST 3 CPM normal/hypernormal GMA was observed in 17 (42%), 18 (67%), and 5 (42%) patients with GP, FD (NGE), and FD (DGE), respectively; and 3 CPM hyponormal in remaining patients in each group. Post-WLST dysrhythmia was comparable.
Conclusions: WLST-electrogastrography coupled with GE study may distinguish between normal/dysrhythmic GMA revealing pathophysiologicalphenotypes of GP and FD. Analysing extent of power change in normogastric, and dysrhythmic frequencies may comprehensively elucidate disease severity.
Keywords: Bradygastria; Electrogastrography; Normogastria; Tachygastria; Water load satiety test.
Conflict of interest statement
Figures




References
LinkOut - more resources
Full Text Sources