

Topological Data Analysis Identified Prognostically-Distinct Phenotypes in Transcatheter Edge-to-Edge Repair Patients
- PMID: 40206628
- PMCID: PMC11975684
- DOI: 10.1016/j.mcpdig.2023.07.002
Topological Data Analysis Identified Prognostically-Distinct Phenotypes in Transcatheter Edge-to-Edge Repair Patients
Abstract
Objective: To identify prognostically distinct phenotype clusters in transcatheter edge-to-edge repair (TEER) patients based on topological data analysis (TDA), which was never used to assess the heterogeneous TEER population.
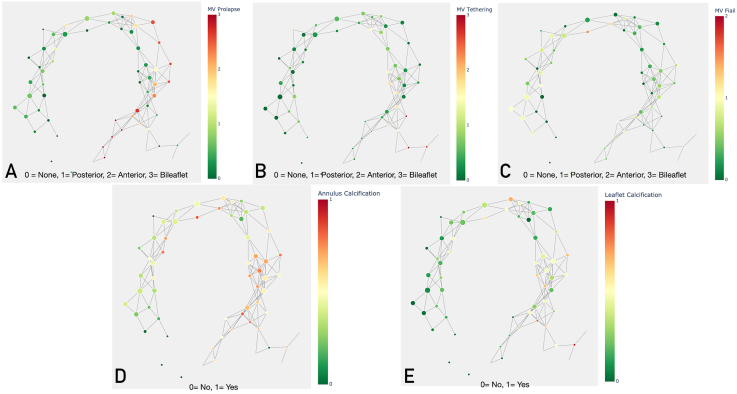
Patients and methods: Patients who underwent TEER (June 2014-September 2020) at Mayo Clinic sites were identified from the institutional database. Thirteen variables were used for TDA. The topological network graph was created using the Python Scikit-TDA Kepler-Mapper package (v. 2.0.1), and clustering was performed at the graph level with Louvain's modularity method. Kaplan-Meier survival analysis was used to assess the all-cause mortality of each cluster.
Result: A total of 389 consecutive patients were included in the final analysis, and 2 major clusters were identified. The mean age was 80.3 ± 8.7 years; 256 (65.8%) were male. Fifty-five (14.5%) patients died during the mean follow-up duration (185 days). Kaplan-Meier analysis showed significant survival differences among the 2 clusters (hazard ratio, 2.70; 95% CI, 1.50-4.87; P=.0005). Cluster 1 (n=227) had moderate or increased residual mitral regurgitation (cluster 0 vs cluster 1: 19.4% vs 41.9%; P<.001) and worse survival performance. Cluster 1 was characterized by worse tricuspid regurgitation severity, higher proportions of patients with atrial fibrillation or flutter, anterior or bileaflet leaflet prolapse, anterior leaflet flail, and mitral annular or leaflet calcification.
Conclusion: TDA can identify prognostically distinct clusters in TEER patients based on mitral valve morphology and clinical risk factors. This simple model can facilitate risk stratification for TEER patients regarding procedural success and survival performance.
© 2023 The Authors.
Conflict of interest statement
The authors report no competing interests.
Figures







References
LinkOut - more resources
Full Text Sources
