

Irreducible Locked Symphysis Pubis Disruption Caused by Incarcerated Urinary Bladder in a 14-year-Old Boy, a Case Report and Review of the Literature
- PMID: 40206637
- PMCID: PMC11980932
- DOI: 10.2147/ORR.S514655
Irreducible Locked Symphysis Pubis Disruption Caused by Incarcerated Urinary Bladder in a 14-year-Old Boy, a Case Report and Review of the Literature
Abstract
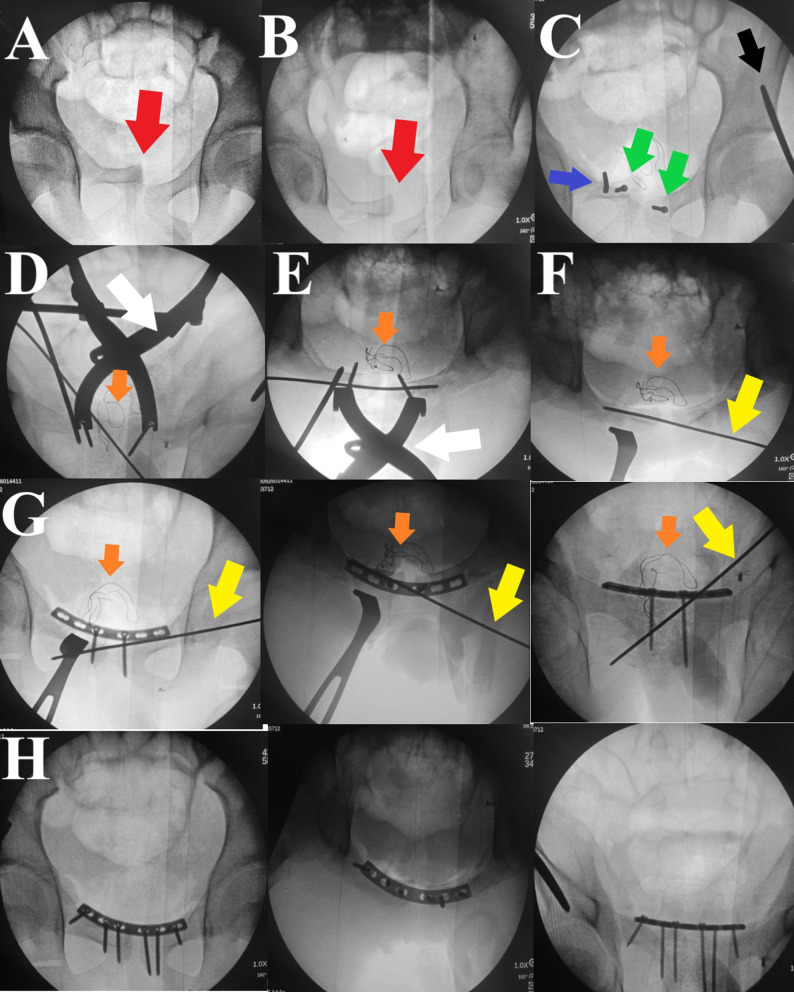
Urinary bladder entrapment or incarceration within pelvic fracture have been described in many reports in the literature, most of which were reported in adult patients. We describe a case of a 14-year-old boy presented with isolated locked symphysis pubis disruption after falling from a height. His initial evaluation was negative for any other associated injuries. The decision was made to treat him surgically by open reduction and internal fixation using a symphyseal plate; however, upon completing the Pfannenstiel incision, the surgeon faced a soft tissue mass hindering bony fragment dissection; upon careful examination, the soft tissue mass turned out to be entrapped urinary bladder within the symphyseal disruption. After careful soft tissue dissection, and with the help of Jungbluth distractor, the disruption was over-distracted, the bladder was freed entirely (which was intact) and reduced to its position, followed by the application of a symphyseal plate in a reduced symphysis pubis position. The patient did well postoperatively, and at three months follow up, the disruption and fracture united, and there were no urinary-related symptoms. Although rare, urinary bladder entrapment within an element of anterior pelvic fracture could be a reason for the difficult reduction; careful evaluation and steady soft tissue dissection are paramount for avoiding undue iatrogenic urinary bladder injury.
Keywords: bladder entrapment; case report; pediatric pelvic fracture.
© 2025 Fergany et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest in this work.
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
