

Real world experience with omission of therapeutic lymph node dissection in clinical stage III malignant melanoma treated with checkpoint or kinase inhibition systemic therapy
- PMID: 40207185
- PMCID: PMC11981639
- DOI: 10.1016/j.soi.2025.100131
Real world experience with omission of therapeutic lymph node dissection in clinical stage III malignant melanoma treated with checkpoint or kinase inhibition systemic therapy
Abstract
Background: Management of clinical stage III melanoma, which historically was treated with surgical therapeutic lymph node dissection (TLND), has changed significantly due to the introduction of effective systemic therapies including immune checkpoint and BRAF/MEK inhibitors. We asked how surgical interventions changed progression free survival and overall survival in this population.
Methods: The Flatiron Health electronic health records database for Advanced Melanoma was queried for patients with clinical stage III melanoma treated between 2018 and 2022 with systemic therapy. Patients were stratified by receipt of TLND.
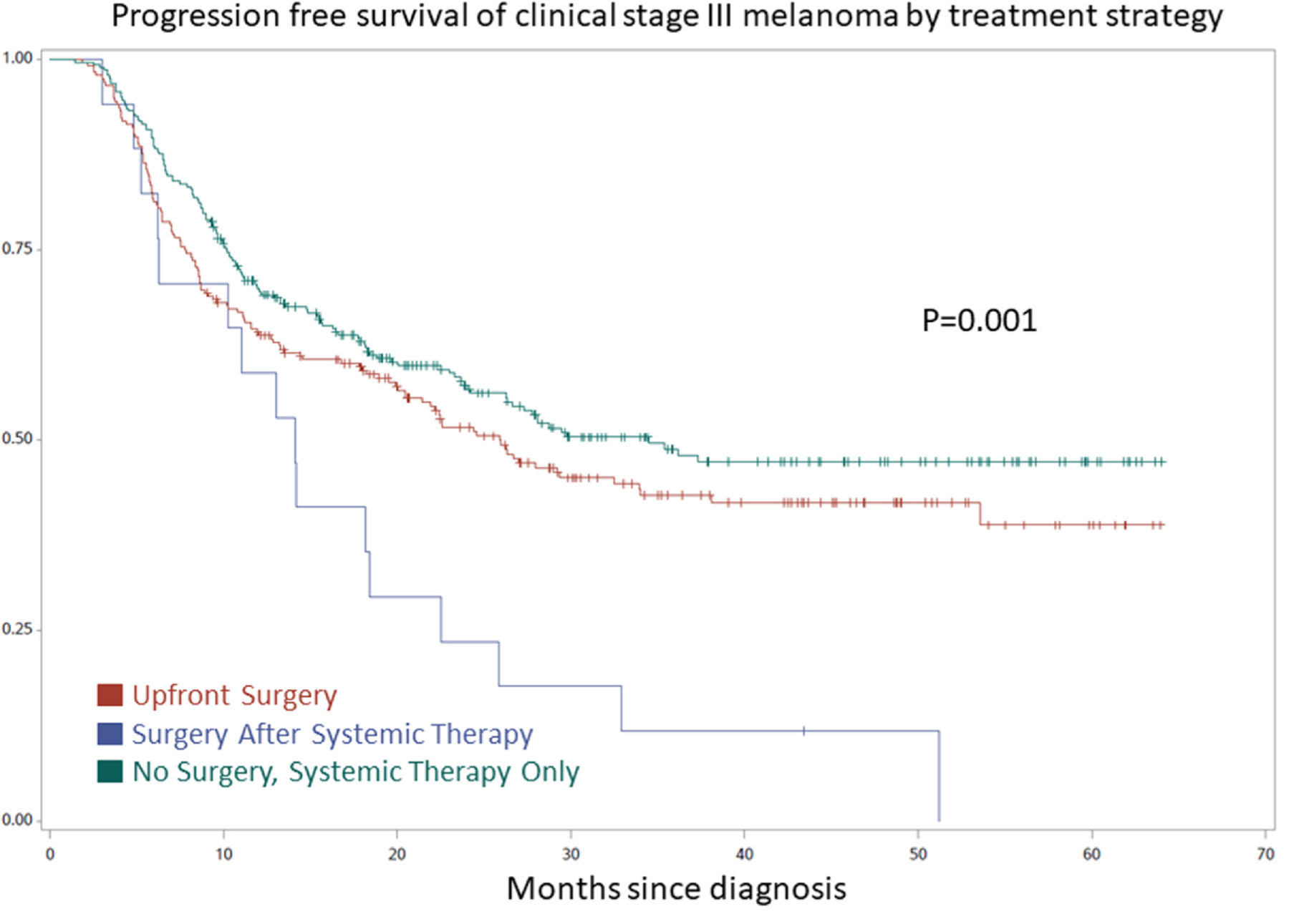
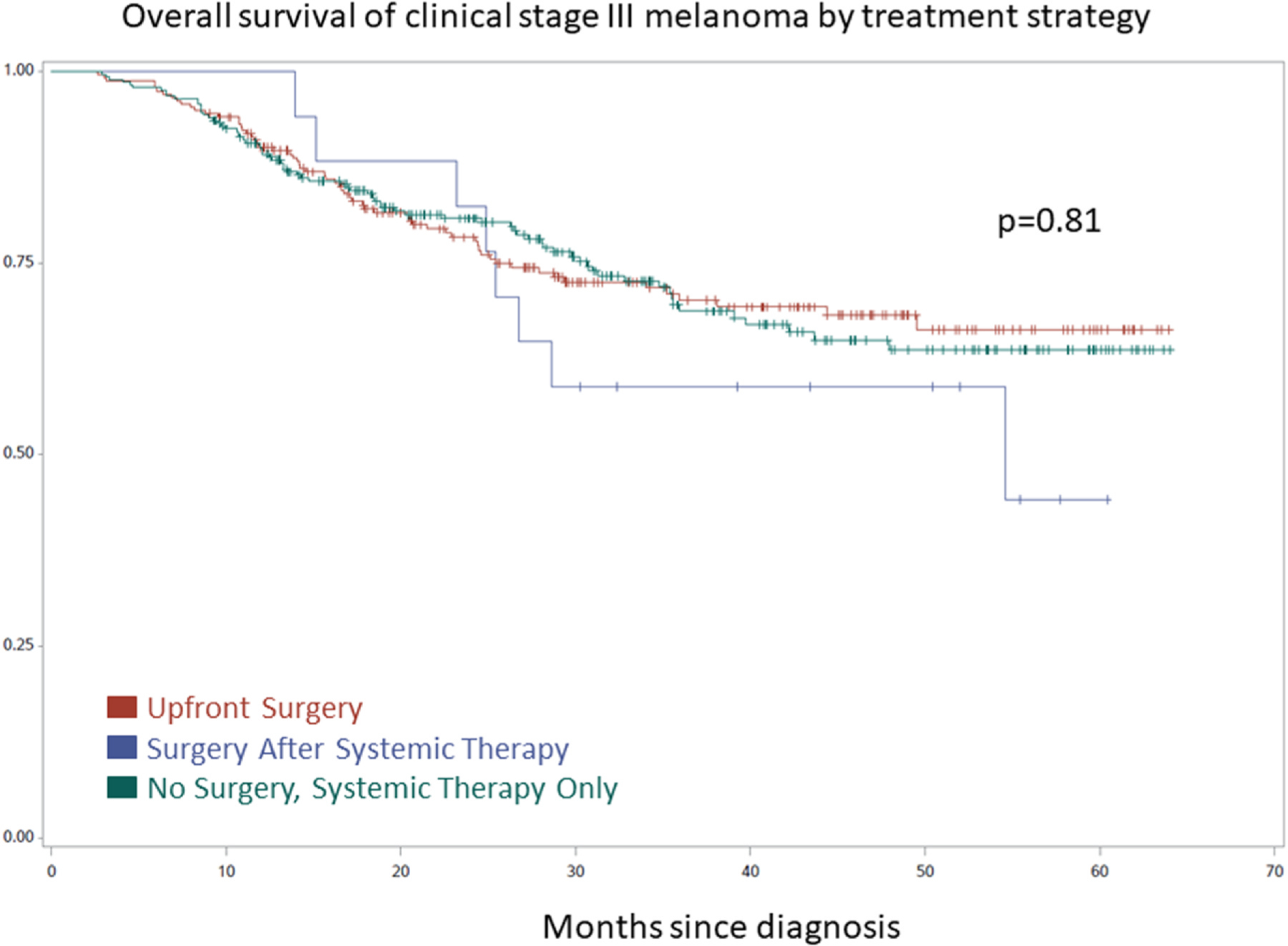
Results: There were 533 patients with clinical stage III melanoma treated with systemic therapy identified; 235 (44.1 %) underwent TLND prior to systemic therapy, 17 (3.2 %) underwent TLND after receipt of systemic therapy, and 281 (52.7 %) received systemic therapy alone and did not have surgery. There were 38.1 % (n = 203) who experienced disease progression at 2 years. Patients in the no surgery group had the best 2-year progression free survival (67.3 %) compared to the upfront surgery (58.3 %) and surgery after systemic therapy groups (23.5 %, p = 0.001), and there was no difference in 2-year overall survival (82.2 % vs 80.0 % vs 82.3 %, p = 0.81). These findings persisted on multivariable analysis.
Conclusions: In this modern era dataset, more than half of patients with clinical stage III melanoma were treated with systemic therapy alone, despite guideline recommendations for TLND. They had superior progression free survival and similar overall survival compared to those also treated with potentially morbid surgery. Randomized data are needed to evaluate appropriate omission of surgery in this patient population.
Keywords: Immune checkpoint inhibitors; Immunotherapy; Lymphadenectomy; Stage III melanoma; Therapeutic lymph node dissection.
Conflict of interest statement
Declaration of Competing Interest Dr. Stewart is a consultant for Merit Medical. Dr. Medina reports Institutional Principal Investigator (institutional funding) for the following: Bristol Myers Squibb, Genentech, Inc., Iovance pharmaceuticals, Merck & Co., Inc., Agenus, Other-Anaveon, Other-Bioatla, Inc, Other-Infla-Rx, Other-Moderna, Other-Replimune, Other-TriSalus, Other-Ultimovacs, Pfizer Inc., Regeneron Pharmactcls, SeaGen, and Immatics. All other authors had nothing to report.
Figures
Similar articles
-
Representativeness of the Index Lymph Node for Total Nodal Basin in Pathologic Response Assessment After Neoadjuvant Checkpoint Inhibitor Therapy in Patients With Stage III Melanoma.JAMA Surg. 2022 Apr 1;157(4):335-342. doi: 10.1001/jamasurg.2021.7554. JAMA Surg. 2022. PMID: 35138335 Free PMC article. Clinical Trial.
-
Impact of personalized response-directed surgery and adjuvant therapy on survival after neoadjuvant immunotherapy in stage III melanoma: Comparison of 3-year data from PRADO and OpACIN-neo.Eur J Cancer. 2025 Jan;214:115141. doi: 10.1016/j.ejca.2024.115141. Epub 2024 Nov 19. Eur J Cancer. 2025. PMID: 39602990 Clinical Trial.
-
The Effect of Neoadjuvant Systemic Therapy on Surgical Outcomes After Lymph Node Dissections for Stage III Melanoma; An Australian Cohort.Ann Surg Oncol. 2024 Aug;31(8):5324-5330. doi: 10.1245/s10434-024-15274-0. Epub 2024 May 18. Ann Surg Oncol. 2024. PMID: 38762644 Free PMC article.
-
Early (sentinel lymph node biopsy-guided) versus delayed lymphadenectomy in melanoma patients with lymph node metastases : personal experience and literature meta-analysis.Cancer. 2010 Mar 1;116(5):1201-9. doi: 10.1002/cncr.24852. Cancer. 2010. PMID: 20066719 Review.
-
[Sentinel node biopsy and lymph node dissection in the era of new systemic therapies for malignant melanoma].Hautarzt. 2019 Nov;70(11):864-869. doi: 10.1007/s00105-019-04491-4. Hautarzt. 2019. PMID: 31605168 Review. German.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials