

doi: 10.1016/j.eats.2024.103246.
eCollection 2025 Mar.
Arthroscopic Exposure for Anterosuperior Rotator Cuff Repair
Affiliations
- PMID: 40207313
- PMCID: PMC11977121
- DOI: 10.1016/j.eats.2024.103246
Item in Clipboard
Arthroscopic Exposure for Anterosuperior Rotator Cuff Repair
Arthrosc Tech.
.
Abstract
Anterosuperior cuff tear involves the subscapularis and supraspinatus and should be analyzed and repaired as a single, large, continuous tear. This presupposes recognition of the complex anatomical anterosuperior shoulder area and a step-by-step approach knowing elements to release and those to preserve. This Technical Note describes a technique for arthroscopic release enabling optimal exposure of the anterosuperior structures as a key step for successful anatomical reconstruction.
© 2024 The Authors.
Figures

Right shoulder, position of arthroscopic portals is outlined before incision. Portal 1, standard posterior portal; portal 2, lateral subacromial portal; portal 3, anterosuperolateral portal; portal 4, anterior (rotator interval) portal. Reprinted with permission.
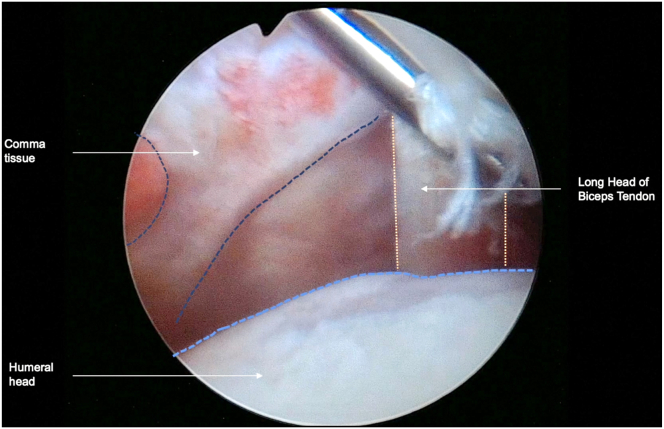
Right shoulder, patient is in the beach-chair position, and scope is in the posterior portal. Once the intra-articular scope has been introduced, the coma sign is directly visualized and identified as the starting point for the procedure. Here, the damaged biceps tendon does not allow tenodesis, and tenotomy is preferred.

Right shoulder, patient is in the beach-chair position, and scope is in the posterior portal with intra-articular view. On the left, comma tissue (asterisk) is grasped through the anterolateral portal, which will reduce the lesion and help to identify upper border of the subscapularis (SSC) and rotator interval (RI). In the central image, traction applied on the comma sign allows debridement of RI with electrocautery device in the lateral portal. On the right, final opening of RI with preservation of comma tissue and visualization of conjoint tendon (CT).

Right shoulder, patient is in the beach-chair position, scope is introduced in the posterior portal with intra-articular visualization, and the shaver is placed at the bursal side of the subscapularis. After intra-articular release and opening of the rotator interval, we can identify the tip of the coracoid (Cor), the coracoacromial ligament (green triangle), and the start of the conjoint tendon (CT). This is a limit that must not be crossed medially, to avoid nerve injury.
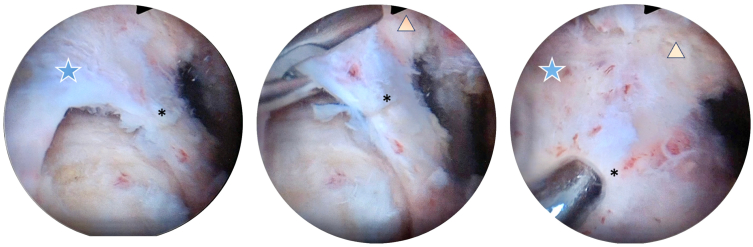
The patient is shown in the beach-chair position, and the scope is in anterolateral portal. On the left side, we can observe the anterolateral tear with supraspinatus (blue star) and comma tissue at the anterior part (asterisk). Then, an arthroscopic grasper from lateral portal is used to reduce the comma tissue and expose the coracohumeral ligament (orange triangle) in the center. On the right, the grasper is used to apply posterolateral traction on the cuff, putting tension on coracohumeral ligament.

The patient is in the beach-chair position, scope in the anterolateral portal; these are the next steps of Fig 5. On the left side, an electrocautery device is used to release the coracohumeral ligament, respecting the supraspinatus tendon (blue star), subscapularis tendon (white star), and the comma tissue (asterisk). Final release of coracohumeral ligament is performed in the central image. On the right side, final aspect of complete release of the anterosuperior tear, maintained reduced by the grasper from lateral portal not in the field of vision here. Green star indicates the superior border of the subscapularis tendon.
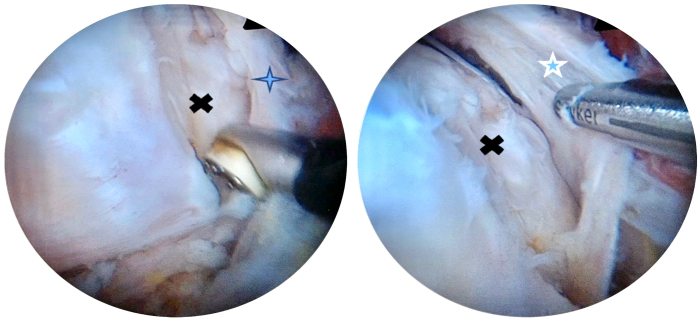
The patient is in the beach-chair position, the scope is in the lateral portal, and the instrumental portal is the anterolateral portal. On the left side, an electrocautery device is used to open the transverse ligament (blue cross) exposing the groove (black X). On the right, comma tissue (blue star) is visualized from articular side, and it will be easier for anatomical reconstruction of these anterolateral cuff tears.

The patient is in the beach-chair position, and the scope is in the lateral portal. After placing an anchor in the lesser tuberosity, we start the repair of the subscapularis (green star) with a Mason-Allen suture placed arthroscopically. In the center, final aspect of the subscapularis repair with preservation of the comma tissue (asterisk). On the right, we finish the repair by the supraspinatus repair (blue star), and it allows a good reduction of the comma tissue.
References
-
- Arai R., Sugaya H., Mochizuki T., Nimura A., Moriishi J., Akita K. Subscapularis tendon tear: An anatomic and clinical investigation. Arthroscopy. 2008;24:997–1004. - PubMed
-
- Lafosse L., Jost B., Reiland Y., Audebert S., Toussaint B., Gobezie R. Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears. J Bone Joint Surg Am. 2007;89:1184–1193. - PubMed
-
- Bennett W.F. Arthroscopic repair of anterosuperior (supraspinatus/subscapularis) rotator cuff tears: A prospective cohort with 2- to 4-year follow-up. Classification of biceps subluxation/instability. Arthroscopy. 2003;19:21–33. - PubMed
-
- Monroe E.J., Flores S.E., Chambers C.C., et al. Patient-reported outcomes after isolated and combined arthroscopic subscapularis tendon repairs. Arthroscopy. 2019;35:1779–1784. - PubMed
LinkOut - more resources
Full Text Sources
