

Arthroscopic Tri-anchor Double-Pulley Suture-Bridge Reduction of Greater Tuberosity Fracture
- PMID: 40207320
- PMCID: PMC11977146
- DOI: 10.1016/j.eats.2024.103263
Arthroscopic Tri-anchor Double-Pulley Suture-Bridge Reduction of Greater Tuberosity Fracture
Abstract
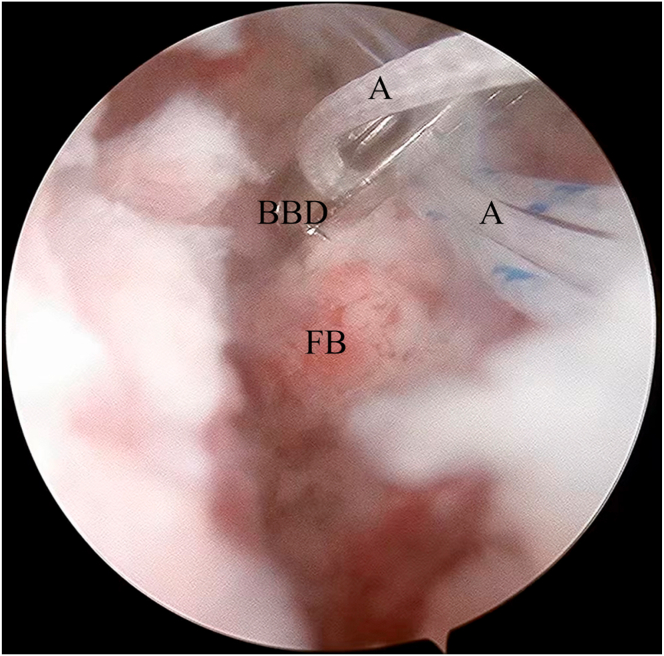
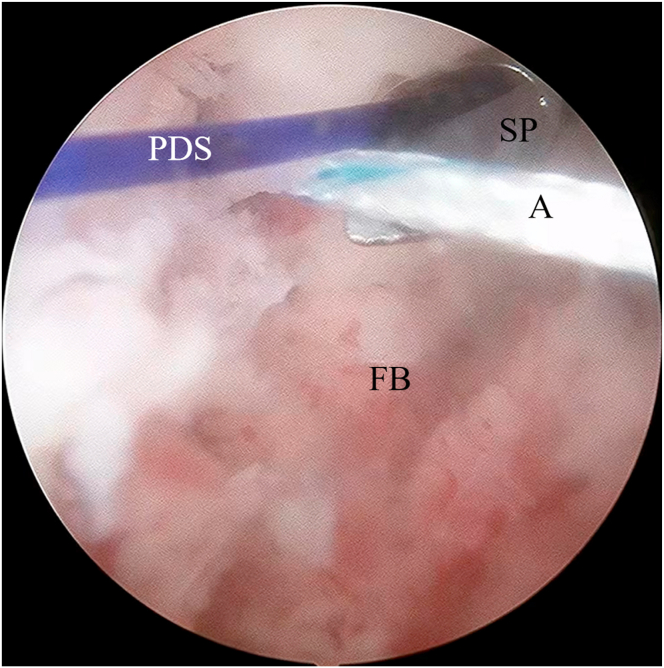
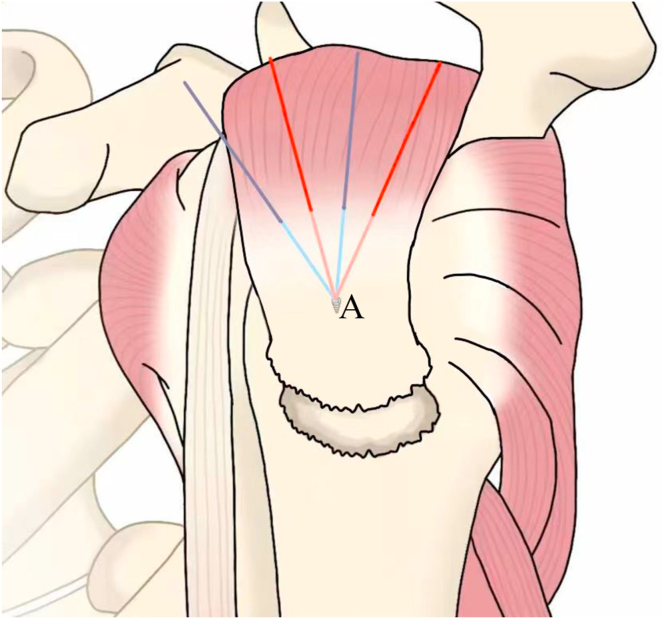
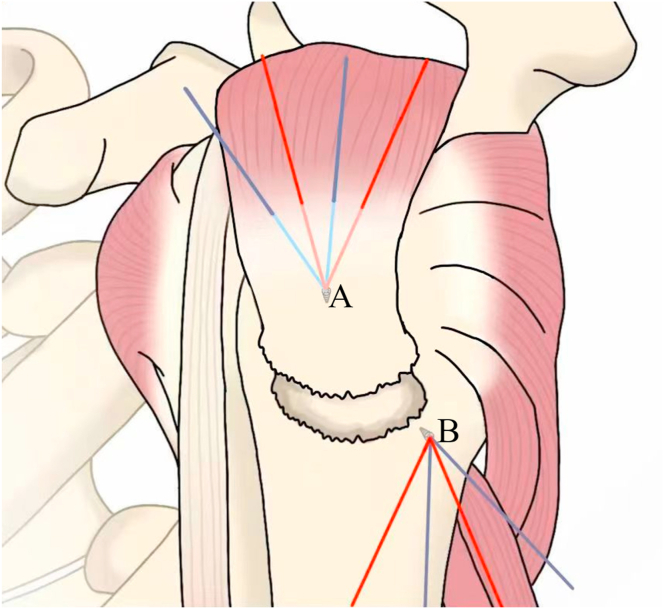
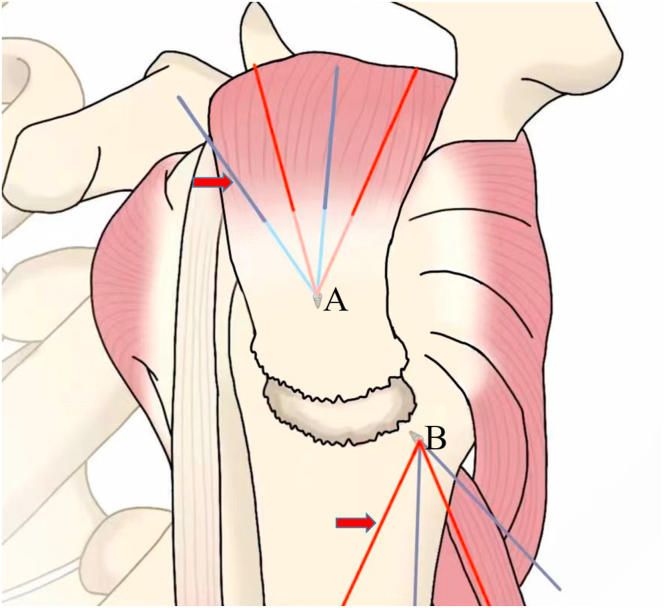
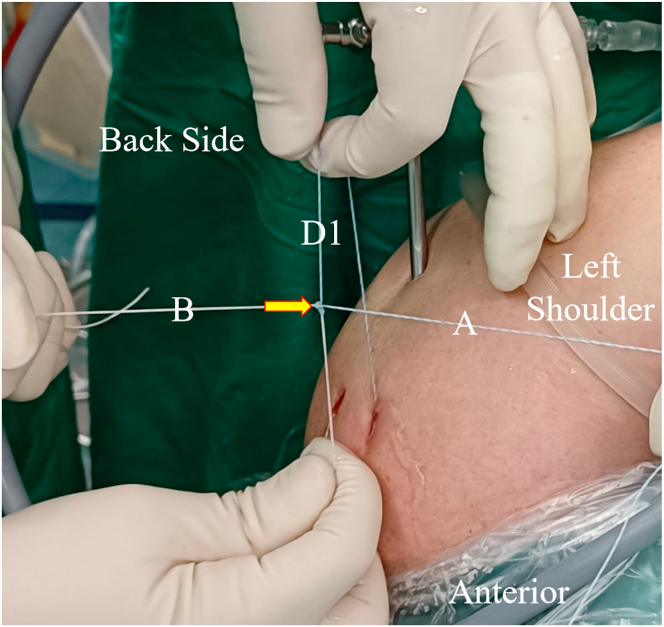
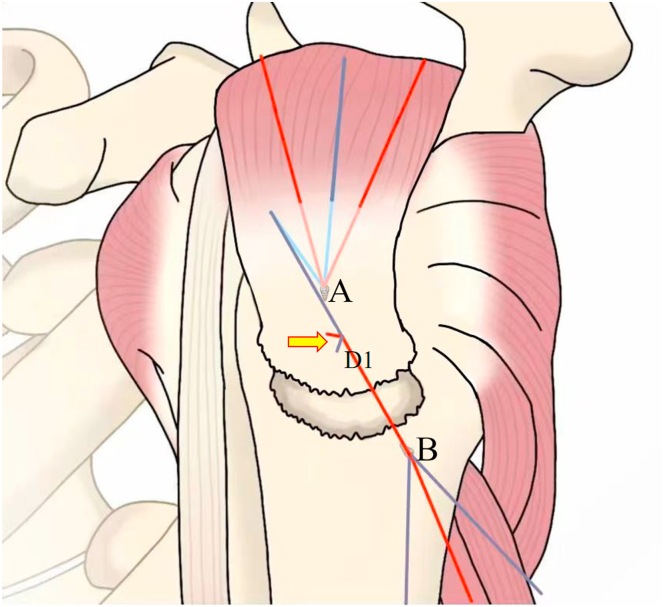
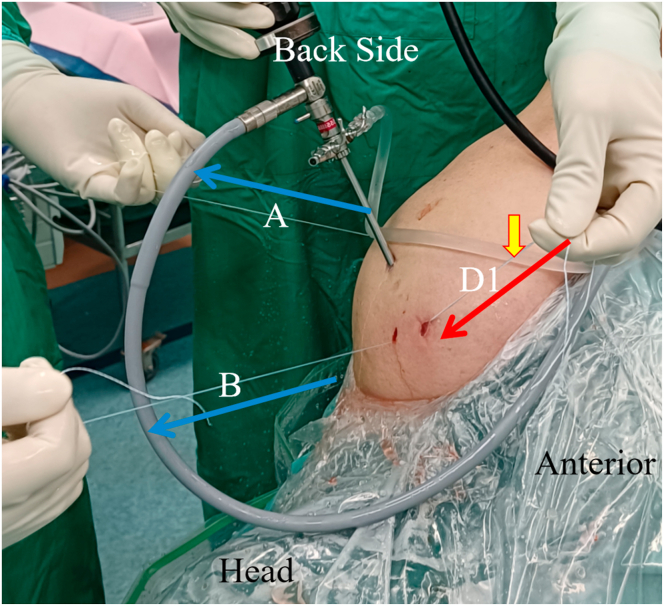
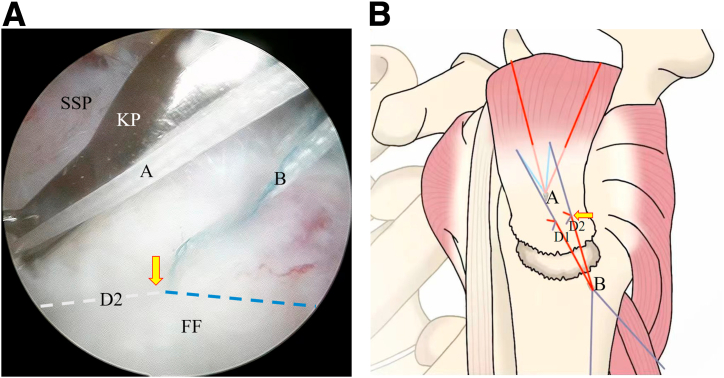
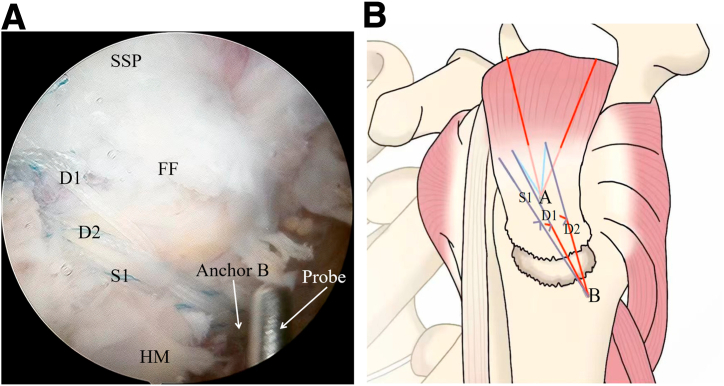
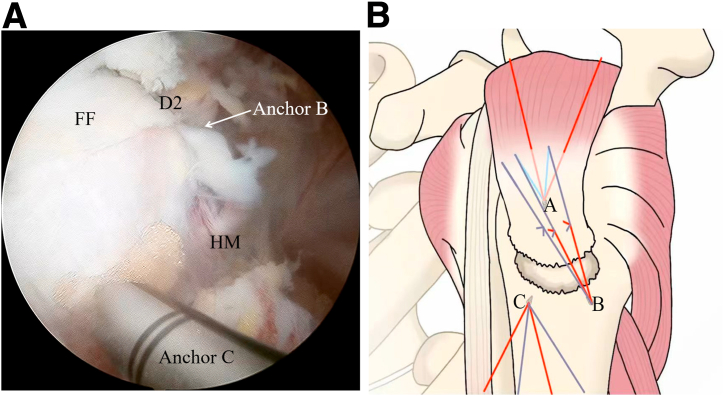
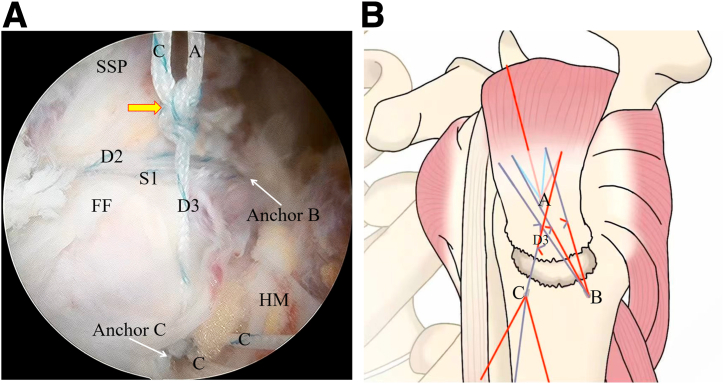
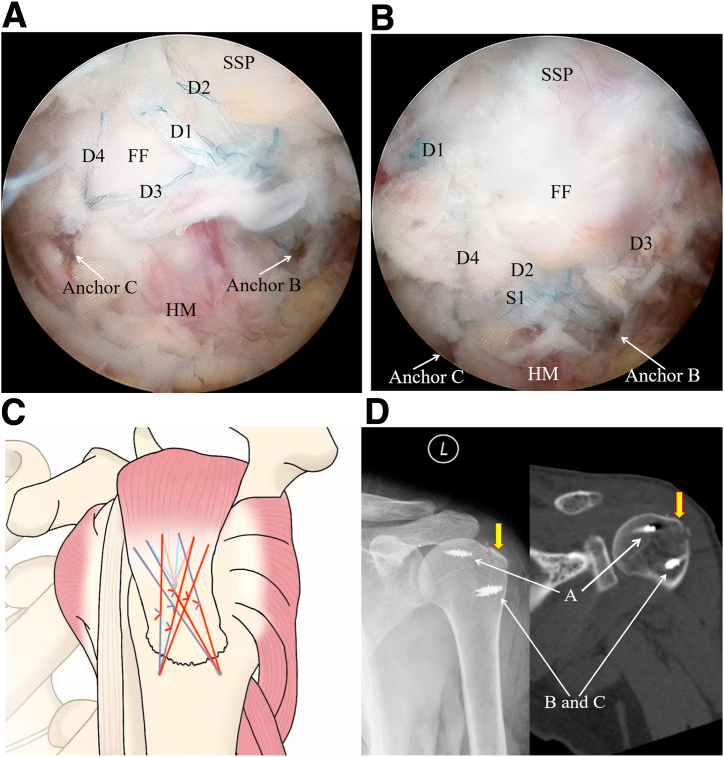
Currently, cannulated screws, plates, and suture bridges are widely applied in the treatment of greater tuberosity fracture; however, further fragmentation of the fracture, risk of loss of fracture reduction, implant impingement, and anchor pullout are the drawbacks. Therefore, we present a pragmatic surgical technique called the arthroscopic tri-anchor double-pulley suture-bridge technique that uses a double-loaded metallic anchor as a lateral-row anchor. In the treatment of greater tuberosity fracture, this hybrid repair including 4 sets of double-pulley suture bridges and 2 sets of single rows can obtain powerful stiffness of the suture construct, the metallic anchor used as a lateral-row anchor can significantly reduce the risk of anchor pullout, the single-row process can lessen the overall surgical time, and implant impingement will not occur postoperatively.
© 2024 The Authors.
Conflict of interest statement
All authors (P.H., X.W., Y.F., Z.X., Z.L., B.P., C.H.) declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Is Arthroscopic Technique Superior to Open Reduction Internal Fixation in the Treatment of Isolated Displaced Greater Tuberosity Fractures?Clin Orthop Relat Res. 2016 May;474(5):1269-79. doi: 10.1007/s11999-015-4663-5. Epub 2016 Jan 4. Clin Orthop Relat Res. 2016. PMID: 26728514 Free PMC article.
-
Arthroscopic Double-Pulley Suture-Bridge Repair of Supraspinatus Tendon Tear.Arthrosc Tech. 2023 Dec 4;13(1):102810. doi: 10.1016/j.eats.2023.08.015. eCollection 2024 Jan. Arthrosc Tech. 2023. PMID: 38312863 Free PMC article.
-
Two Techniques for Treating Medium-Sized Supraspinatus Tears: The Medially Based Single-Row Technique and the Suture Bridge Technique.JBJS Essent Surg Tech. 2021 Jun 8;11(2):e20.00004. doi: 10.2106/JBJS.ST.20.00004. eCollection 2021 Apr-Jun. JBJS Essent Surg Tech. 2021. PMID: 34277130 Free PMC article.
-
Soft tissue tenodesis of the long head of the biceps tendon associated to the Roman Bridge repair.BMC Musculoskelet Disord. 2008 Jun 4;9:78. doi: 10.1186/1471-2474-9-78. BMC Musculoskelet Disord. 2008. PMID: 18533031 Free PMC article. Review.
-
Surgical Management of Comminuted, Displaced Greater Tuberosity Fractures: A New Technique of Subacromial Spacer on Top of Double-Row Suture Anchor Fixation.Joints. 2018 Oct 31;6(3):211-214. doi: 10.1055/s-0038-1675162. eCollection 2018 Sep. Joints. 2018. PMID: 30582110 Free PMC article. Review.
References
-
- Maman E., Dolkart O., Chechik O., et al. Arthroscopic findings of coexisting lesions with greater tuberosity fractures. Orthopedics. 2014;37:e272–e277. - PubMed
-
- Ji J.H., Shafi M., Song I.S., Kim Y.Y., McFarland E.G., Moon C.Y. Arthroscopic fixation technique for comminuted, displaced greater tuberosity fracture. Arthroscopy. 2010;26:600–609. - PubMed
-
- Green A., Izzi J., Jr. Isolated fractures of the greater tuberosity of the proximal humerus. J Shoulder Elbow Surg. 2003;12:641–649. - PubMed
-
- Park S.E., Jeong J.J., Panchal K., Lee J.Y., Min H.K., Ji J.H. Arthroscopic-assisted plate fixation for displaced large-sized comminuted greater tuberosity fractures of proximal humerus: A novel surgical technique. Knee Surg Sports Traumatol Arthrosc. 2016;24:3892–3898. - PubMed
LinkOut - more resources
Full Text Sources
