

Neurosurgical management for chronic and end-of-life pain in children: A systematic review
- PMID: 40207462
- PMCID: PMC11983359
- DOI: 10.1111/papr.70034
Neurosurgical management for chronic and end-of-life pain in children: A systematic review
Abstract
Introduction: Chronic and end-of-life pain in children is underreported and undermanaged. Current guidelines for pediatric chronic pain include medical and interventional modalities; however, the inclusion of neurosurgical treatments is uncommon and inconsistent. This systematic review presents the literature, and we provide recommendations for the role of neurosurgical procedures in treating chronic and end-of-life pain in children.
Methods: A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) guidelines using three databases: PubMed, Embase, and Scopus. We included 40 studies presenting neurosurgical procedures for the treatment of chronic and end-of-life pain in children.
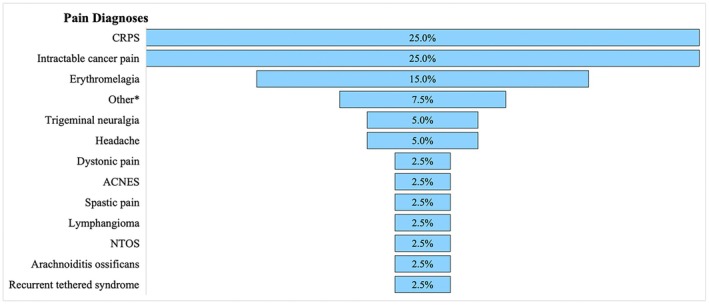
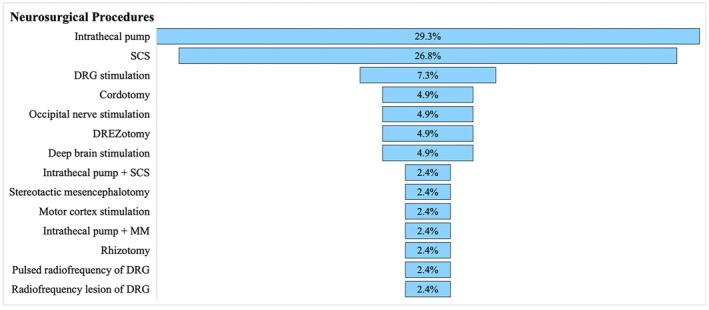
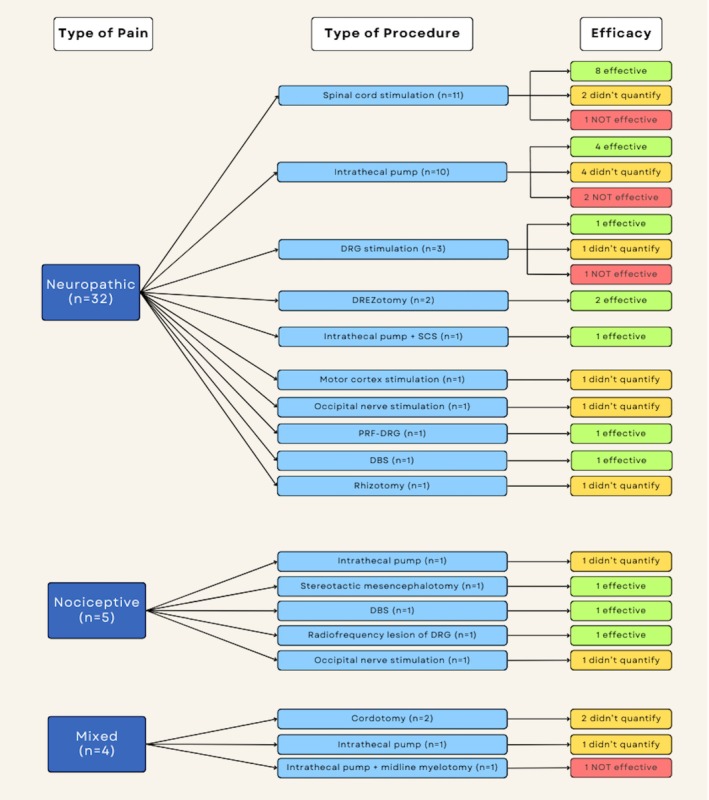
Results: Thirty-one (77.5%) manuscripts focused on the treatment of neuropathic pain, five (12.5%) focused on nociceptive pain, and four (10%) treated mixed pain conditions. The most common neurosurgical procedure was intrathecal opioid therapy via pump placement (29.3%), followed by spinal cord stimulation (26.8%). Neuropathic pain syndromes were primarily treated with neurostimulation (58%), demonstrating good efficacy. Ablative procedures (40%) were most effective for nociceptive pain syndromes. Both chordotomy and intrathecal pumps provided subjective pain relief for mixed pain syndromes. The quantification of procedural efficacy, including pain outcomes and grading scales, varied significantly across studies.
Conclusion: Neurosurgical treatments for chronic pediatric pain are safe, although broad efficacy cannot be determined due to sparse literature and inadequately quantified pain responses. Guidelines for escalating chronic and end-of-life pain management in pediatric patients should be updated to include neurosurgical treatments and appropriate outcome scales. Focused research on appropriate patients, available neurosurgical therapies, and pediatric outcomes is warranted.
Keywords: analgesia; intrathecal; neurosurgical procedures; pediatric pain; spinal cord; stimulation.
© 2025 The Author(s). Pain Practice published by Wiley Periodicals LLC on behalf of World Institute of Pain.
Conflict of interest statement
Jeffrey S. Raskin is a paid consultant to Iota, Synergia, BlackRock Neurotech, and Medtronic. The other authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
[Neurosurgical treatment of chronic pain].Rev Prat. 2013 Jun;63(6):805-9. Rev Prat. 2013. PMID: 23923757 Review. French.
-
Spinal cord stimulation for treatment of chronic neuropathic pain in adolescent patients: a single-institution series, systematic review, and individual participant data meta-analysis.Neurosurg Focus. 2022 Oct;53(4):E13. doi: 10.3171/2022.7.FOCUS22330. Neurosurg Focus. 2022. PMID: 36183181
-
[Neurosurgical treatments for pain].Rev Med Brux. 2012 Sep;33(4):359-66. Rev Med Brux. 2012. PMID: 23091942 Review. French.
-
Comprehensive Evidence-Based Guidelines for Implantable Peripheral Nerve Stimulation (PNS) in the Management of Chronic Pain: From the American Society Of Interventional Pain Physicians (ASIPP).Pain Physician. 2024 Nov;27(S9):S115-S191. Pain Physician. 2024. PMID: 39565237
-
The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the Neuromodulation Appropriateness Consensus Committee.Neuromodulation. 2014 Aug;17(6):515-50; discussion 550. doi: 10.1111/ner.12208. Neuromodulation. 2014. PMID: 25112889
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
