

Influence of Echocardiographic Criteria on the Prevalence and Prognostic Implication of Left Ventricular Hypertrophy: A Nationwide Population-Based Study
- PMID: 40207478
- PMCID: PMC12132816
- DOI: 10.1161/JAHA.124.038108
Influence of Echocardiographic Criteria on the Prevalence and Prognostic Implication of Left Ventricular Hypertrophy: A Nationwide Population-Based Study
Abstract
Background: Echocardiographic criteria of left ventricular hypertrophy (LVH) recommended in the international guidelines are derived from a White population, which could be less accurate in estimating LVH burden in other ethnic groups. Given that LVH is an important prognostic factor, assessing its burden using ethnically specific criteria has important implications. We sought to evaluate the prevalence and prognostic implications of LVH based on the EMINCA (Echocardiographic Measurements in Normal Chinese Adults) study criteria and the international guidelines.
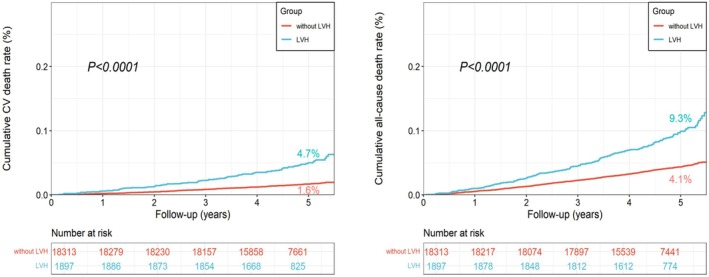
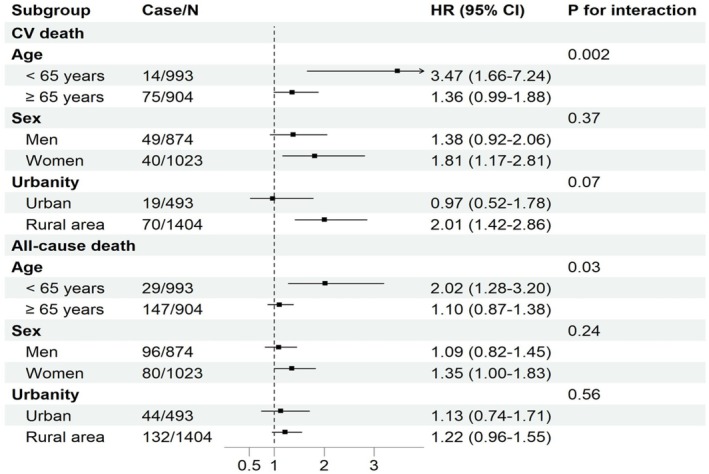
Methods and results: Nationally representative populations aged ≥35 years (n=20 210; mean age, 56.0 years; 53.3% women) were enrolled from the China Hypertension Survey 2012 to 2015. The EMINCA study criteria for LVH were left ventricular mass index >109 g/m2 for men and >105 g/m2 for women; and the international guidelines criteria were left ventricular mass index >115 g/m2 for men and >95 g/m2 for women. Prevalence of LVH defined by the EMINCA study and international guidelines was 8.3% (≈56.8 million) and 11.7% (≈80.1 million), respectively. LVH defined by the EMINCA study was associated with adjusted hazard ratio (HR) of 1.55 (95% CI, 1.19-2.01; P<0.001) for cardiovascular death and 1.14 (95% CI, 0.95-1.37; P=0.16) for all-cause death. LVH defined by the international guidelines was associated with adjusted HR of 1.31 (95% CI, 1.00-1.72; P=0.047) for cardiovascular death and 1.12 (95% CI, 0.94-1.34; P=0.22) for all-cause death.
Conclusions: LVH diagnosis based on both criteria was independently associated with cardiovascular death. However, the prevalence of LVH in a general Chinese population varies significantly by the echocardiographic criteria.
Keywords: left ventricular hypertrophy; prevalence; prognosis.
Conflict of interest statement
None.
Figures
Similar articles
-
Obesity and Risk of Incident Left Ventricular Hypertrophy in Community-Dwelling Populations With Hypertension: An Observational Study.J Am Heart Assoc. 2024 Jun 18;13(12):e033521. doi: 10.1161/JAHA.123.033521. Epub 2024 Jun 6. J Am Heart Assoc. 2024. PMID: 38842284 Free PMC article.
-
Prevalence and risk factors for left ventricular hypertrophy and left ventricular geometric abnormality in the patients with hypertension among Han Chinese.Chin Med J (Engl). 2012 Jan;125(1):21-6. Chin Med J (Engl). 2012. PMID: 22340460
-
Sex-Specific Association of Left Ventricular Hypertrophy With Cardiovascular Events in High-Risk of Cardiovascular Disease Population: Findings From the Sub-Cohort of China PEACE Million Persons Project.J Clin Hypertens (Greenwich). 2025 May;27(5):e70072. doi: 10.1111/jch.70072. J Clin Hypertens (Greenwich). 2025. PMID: 40400489 Free PMC article.
-
Targeting Concentric Left Ventricular Hypertrophy in Obstructive Sleep Apnea Syndrome. A Meta-analysis of Echocardiographic Studies.Am J Hypertens. 2020 Apr 1;33(4):310-315. doi: 10.1093/ajh/hpz198. Am J Hypertens. 2020. PMID: 31863113
-
Why is left ventricular hypertrophy so predictive of morbidity and mortality?Am J Med Sci. 1999 Mar;317(3):168-75. doi: 10.1097/00000441-199903000-00006. Am J Med Sci. 1999. PMID: 10100690 Review.
References
-
- Antikainen RL, Peters R, Beckett NS, Fagard RH, Wang JG, Rajkumar C, Bulpitt CJ. Left ventricular hypertrophy is a predictor of cardiovascular events in elderly hypertensive patients: hypertension in the very elderly trial. J Hypertens. 2016;34:2280–2286. doi: 10.1097/hjh.0000000000001073 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
