

C-reactive protein-to-albumin ratio is associated with mortality after transcatheter tricuspid valve repair
- PMID: 40208300
- PMCID: PMC12202701
- DOI: 10.1007/s00392-025-02641-4
C-reactive protein-to-albumin ratio is associated with mortality after transcatheter tricuspid valve repair
Abstract
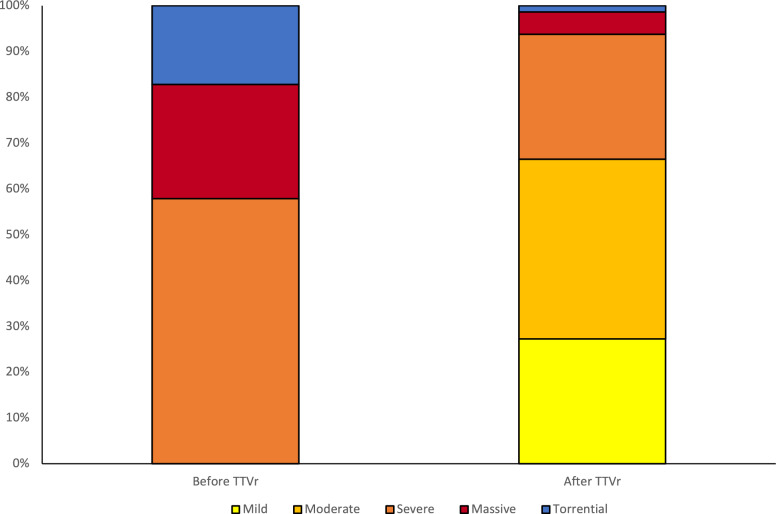
Background: Transcatheter tricuspid valve repair (TTVr) is a treatment option for tricuspid regurgitation (TR) in patients with high surgical risk. Given the heterogeneity in clinical benefit, there is a need for markers to assess mortality risk in patients undergoing TTVr. The C-reactive protein (CRP)/albumin ratio (CAR) is a marker of systemic inflammation and reduced nutritional status, which can both occur in TR.
Methods: Consecutive patients undergoing TTVr at a tertiary care center were retrospectively analyzed. Serum CRP and albumin were collected at baseline. Intraprocedural success (IS) was defined according to TVARC criteria. The primary outcome of all-cause mortality was assessed up to 2 years after TTVr.
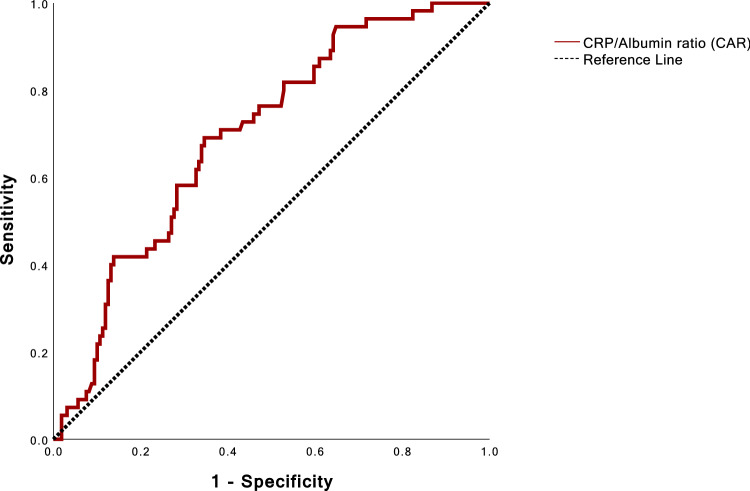
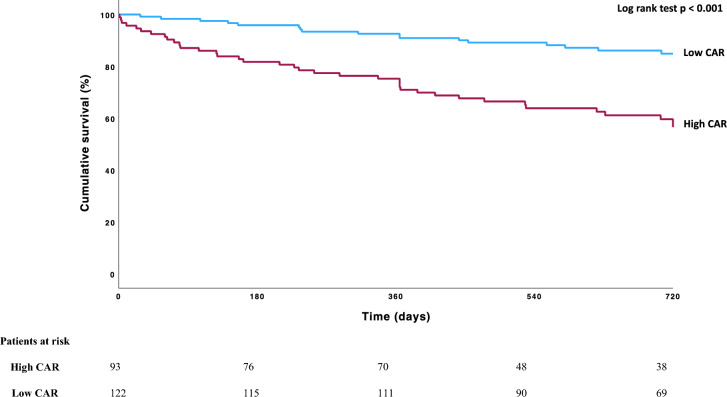
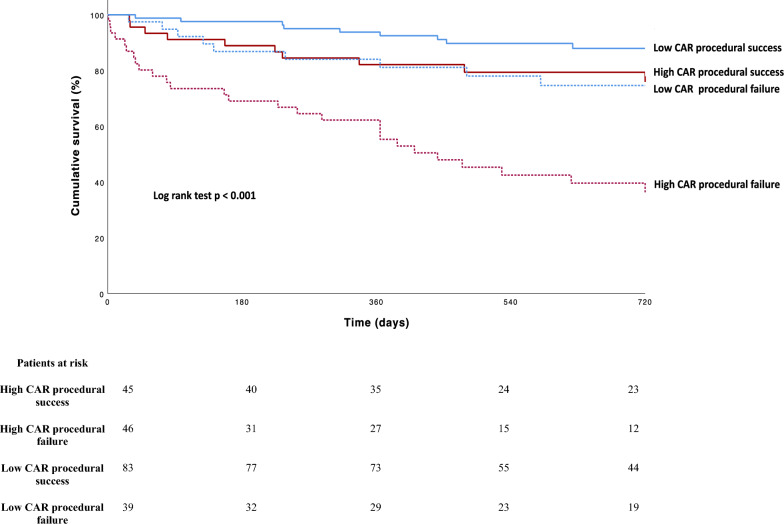
Results: A total of 215 patients (69% females, median age 80 years) were identified. IS was achieved in 61% of patients. AUC of CAR for 2-year mortality was 0.695, with an optimal threshold of 1.2945 (Youden index) dividing patients in high CAR (n = 93) and low CAR (n = 122) groups. In the high CAR group, the primary endpoint occurred more frequently (43% vs 15%, p < 0.001) and significantly higher right atrial pressure, worse renal function, and less IS during TTVr were observed. High CAR was independently associated with an increased mortality risk even when adjusted for renal and liver function, right-ventricular function, and procedural failure (HR 2.188; 95%CI 1.2-3.9; p = 0.011).
Conclusion: Higher CAR reflects patients with advanced right-heart failure and extracardiac organ damage and is associated with mortality after TTVr. CAR is derived from readily available parameters and may be useful additive to established risk scores.
Keywords: Biomarker; Inflammation; Malnutrition; Right heart failure; Transcatheter tricuspid valve repair; Tricuspid regurgitation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: KF, LM, TG, JA, MS, PvS, and JvS report no relevant disclosures. CI and MIK have received travel support by Abbott and Edwards Lifesciences and consultant honoraria by Abbott Vascular and Edwards Lifesciences. SB has received an unrestricted research grant for the MATTERHORN trial—Abbott Vascular and consultant honoraria from Edwards Lifesciences. RP has a speaker engagement with Abbott Vascular and consultant for Edwards Lifesciences.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
