

Misclassification of malaria as pneumonia in children in sub-Saharan Africa
- PMID: 40209071
- PMCID: PMC11984459
- DOI: 10.1093/ije/dyaf040
Misclassification of malaria as pneumonia in children in sub-Saharan Africa
Abstract
Background: The World Health Organization (WHO) clinical case definitions for pneumonia were designed to prioritize sensitivity over specificity. In sub-Saharan Africa, the disease that is most likely to be misclassified as pneumonia is Plasmodium falciparum malaria.
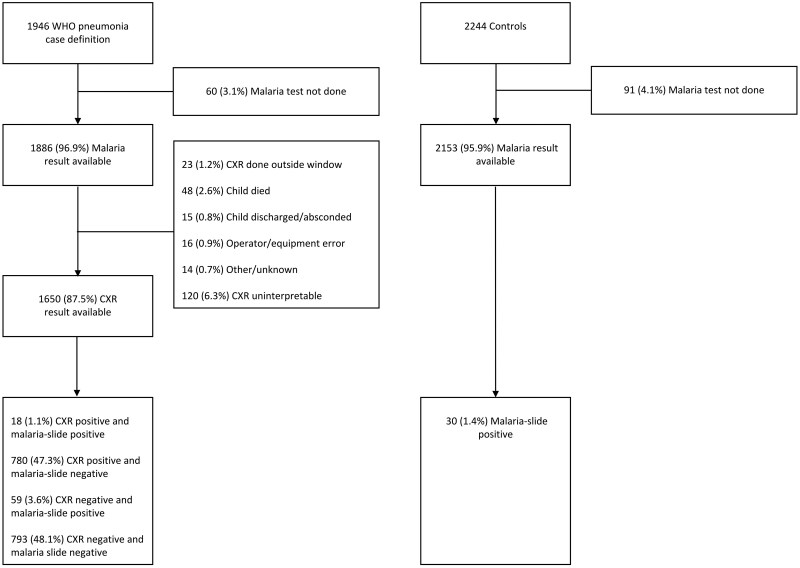
Methods: By using chest X-ray positivity as an indicator for pneumonia, we estimated the extent of pneumonia misclassification due to malaria in the Pneumonia Etiology Research for Child Health (PERCH) study. Additionally, we developed a simple model to predict the proportion of pneumonia cases as defined by the WHO that could be attributed to malaria in settings with varying levels of malaria parasitaemia prevalence.
Results: In the PERCH study, the prevalence of malaria parasitaemia was low (4.7% among WHO pneumonia cases and 1.4% among controls) and we estimate that only 2.5% of WHO pneumonia cases were misclassified. However, when assuming a prevalence of malaria parasitaemia of 24%, corresponding to the average for malaria-endemic areas in Africa, we estimate that 28% of WHO pneumonia cases are misclassified. Among malaria-slide-positive WHO pneumonia cases in PERCH, lower chest wall indrawing [adjusted odds ratio (aOR) =18.1, 95% confidence interval (95% CI): 1.9, 175.8, P = 0.012], crackles on chest auscultation (aOR = 13.1, 95% CI: 1.4, 127.4, P = 0.027), and nasal flaring (aOR = 5.9, 95% CI: 1.1, 32.8, P = 0.041) were associated with chest X-ray positivity.
Conclusion: In settings that are typical of sub-Saharan Africa, we predict that one-quarter of WHO-defined pneumonia cases are malaria rather than pneumonia. Among children with WHO pneumonia who also test positive for malaria parasitaemia, clinical features that favour pneumonia include lower chest wall indrawing, nasal flaring, and crackles on chest auscultation.
Keywords: malaria; misclassification; pneumonia.
© The Author(s) 2025. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures


Comment in
-
Commentary: Navigating symptom and diagnostic overlap in pneumonia and malaria: insights from the field from the PERCH Study.Int J Epidemiol. 2025 Apr 12;54(3):dyaf063. doi: 10.1093/ije/dyaf063. Int J Epidemiol. 2025. PMID: 40441860 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
