

Accelerating inflammatory resolution in humans to improve endothelial function and vascular health: Targeting the non-canonical pathway for NO
- PMID: 40209616
- PMCID: PMC12005330
- DOI: 10.1016/j.redox.2025.103592
Accelerating inflammatory resolution in humans to improve endothelial function and vascular health: Targeting the non-canonical pathway for NO
Abstract
Background: Chronic cardiovascular diseases (CVD) are characterised by low-grade systemic inflammation in part due to reduced nitric oxide (NO) bioavailability associated with endothelial dysfunction. Bioavailability of NO can be enhanced by activation of the non-canonical pathway, through increased dietary inorganic nitrate consumption with the potential to attenuate inflammation.
Methods: We sought to determine whether dietary inorganic nitrate influences the inflammatory response in models of localised (cantharidin-induced blisters) and systemic inflammation (typhoid vaccine), in healthy male volunteers and conducted two clinical trials; Blister-NITRATE and Typhoid-NITRATE respectively.
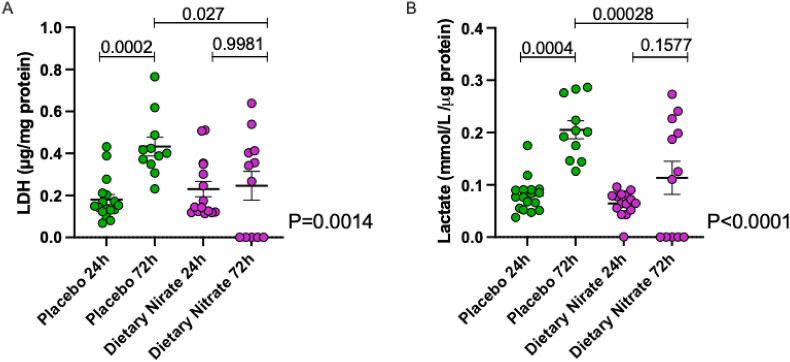
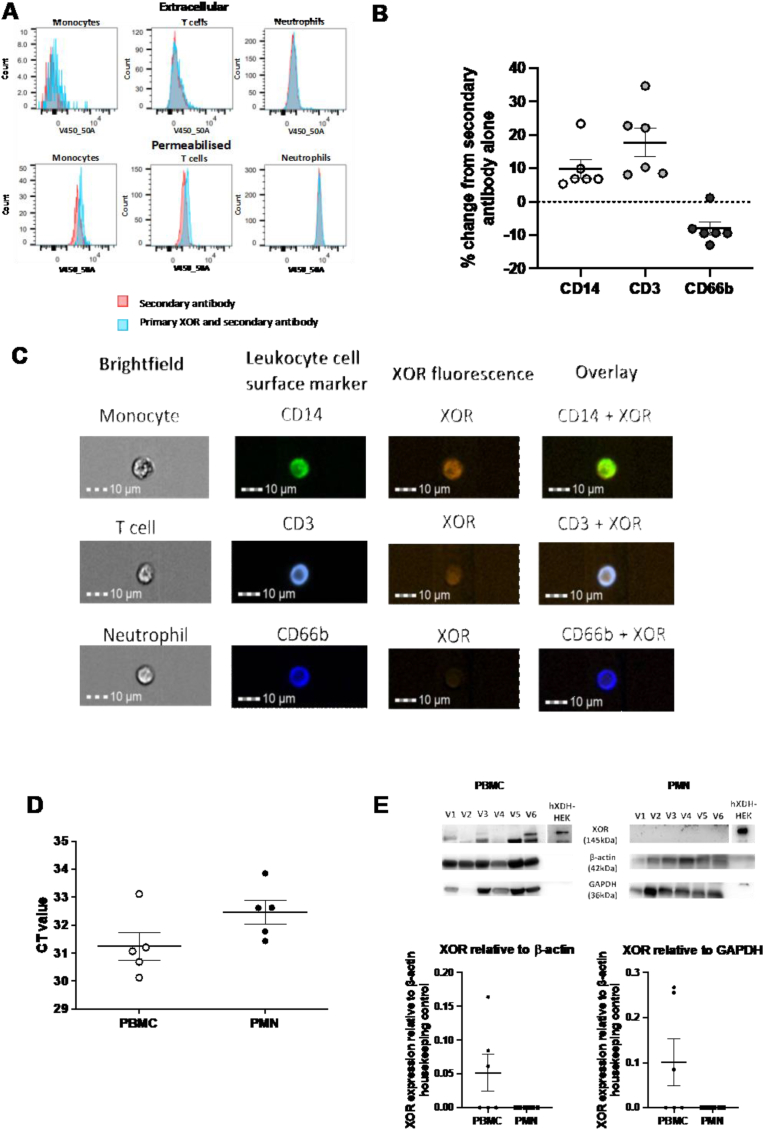
Results: We show that dietary nitrate attenuates endothelial dysfunction following typhoid vaccine administration and accelerates resolution of cantharidin-induced blisters. Both phenomena were associated with an increased level of pro-resolving mediators consequent to a reduction in the expression and activity of pro-inflammatory monocytes. Moreover, we show that leukocytes of the monocyte lineage express the nitrite reductase XOR, that may drive localised nitrite reduction to elevate NO (and cGMP) to drive the protective phenotype.
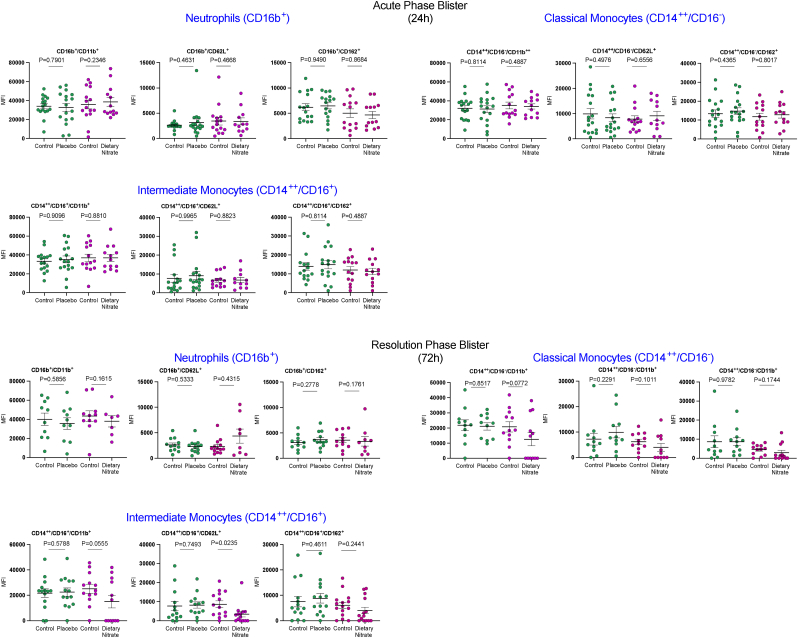
Conclusions: Inorganic nitrate improves endothelial function in the setting of systemic inflammation. Whilst the immediate inflammatory response appeared unaffected by inorganic nitrate treatment, during the resolution phase of the acute inflammatory response lower levels of pro-inflammatory classical inflammatory and intermediate monocytes and attenuated levels of inflammatory cytokines and chemokines were evident. We propose that this reflects a pro-resolution phenotype that may be of potential therapeutic benefit in patients with established CVD.
Clinical trial registration: URL: https://www.
Clinicaltrials: gov; unique identifiers NCT02715635, NCT03183830.
Keywords: Blister; Endothelium; Inflammation; Inorganic; Nitrate; Typhoid.
Copyright © 2025 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Prof A Ahluwalia is a Director of Heartbeet Ltd and IoNa Therapeutics. A Ahluwalia holds two relevant patents: WO2024160924A1; WO2024160921A1.
Figures





References
-
- Kohchi K., Takebayashi S., Hiroki T., Nobuyoshi M. Significance of adventitial inflammation of the coronary artery in patients with unstable angina: results at autopsy. Circulation. 1985;71(4):709–716. - PubMed
-
- Zhao T.X., Mallat Z. Targeting the immune system in atherosclerosis: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2019;73(13):1691–1706. - PubMed
-
- Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524–533. - PubMed
-
- Cai H., Harrison D.G. Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circ. Res. 2000;87:840–844. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
