

The usefulness of different imaging modalities in mandibular osteonecrosis and osteomyelitis diagnosis
- PMID: 40210732
- PMCID: PMC11986015
- DOI: 10.1038/s41598-025-96910-x
The usefulness of different imaging modalities in mandibular osteonecrosis and osteomyelitis diagnosis
Abstract
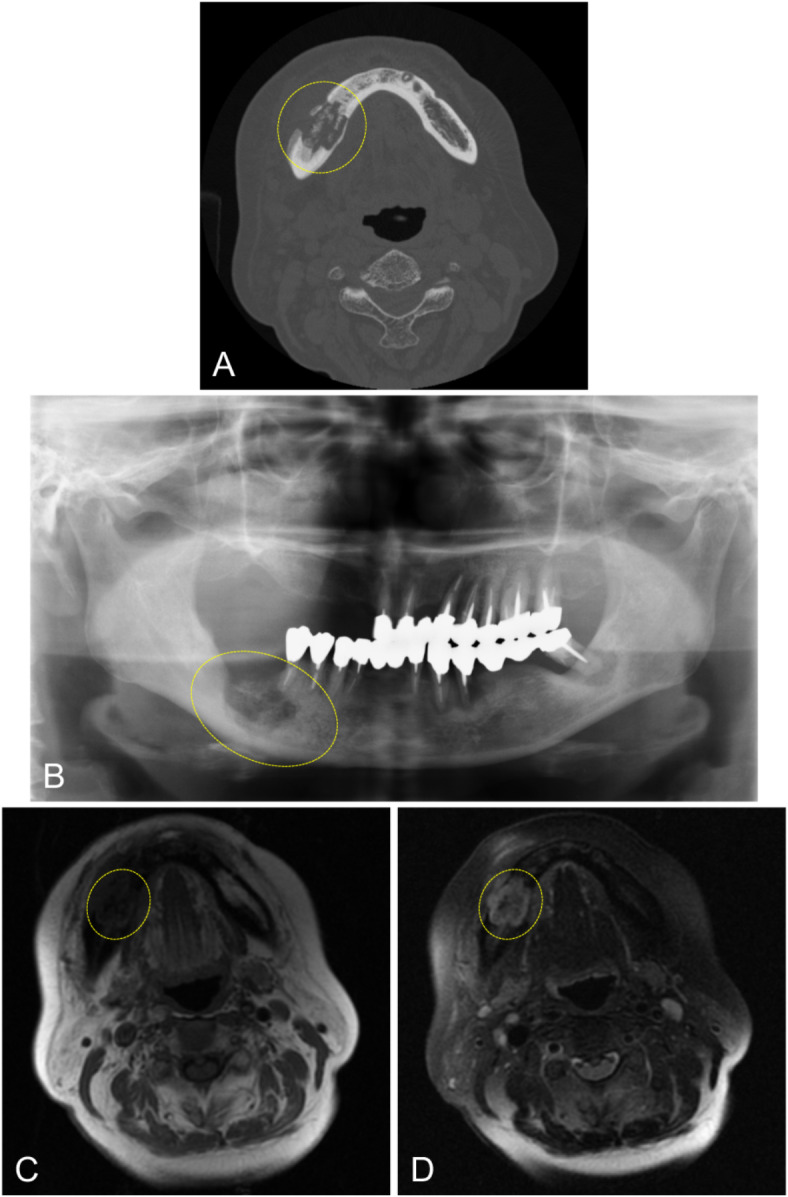
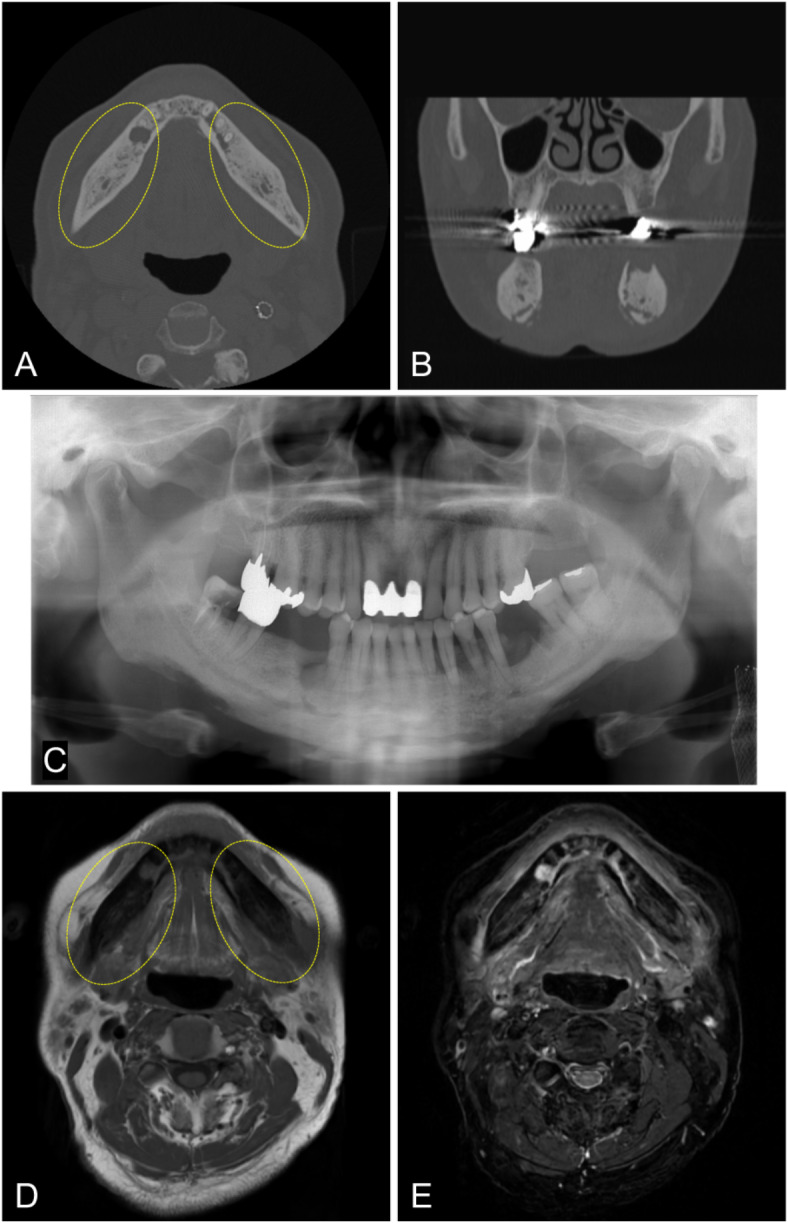
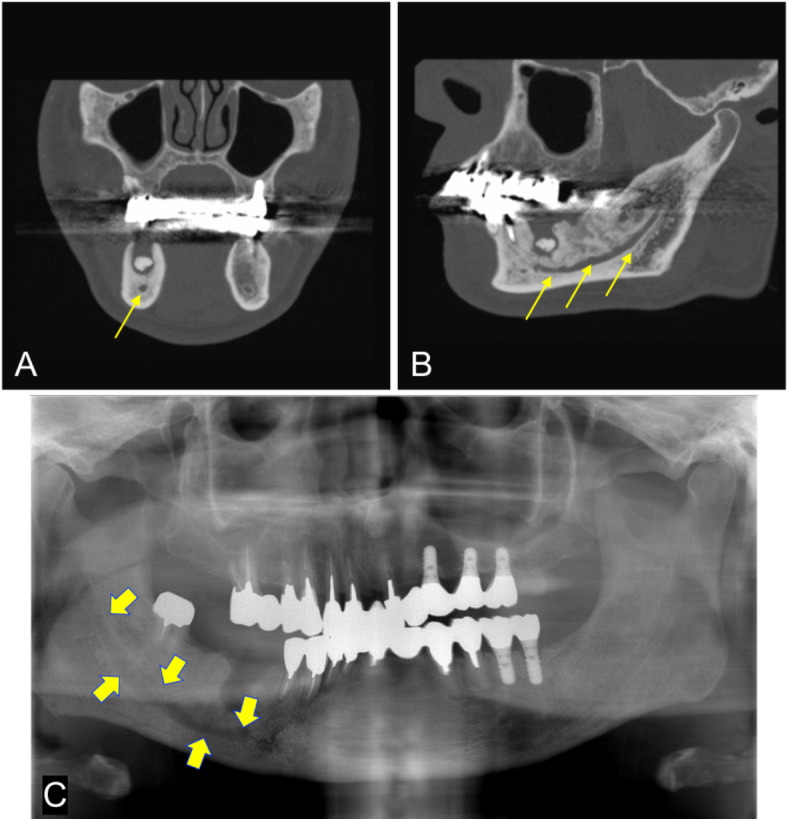
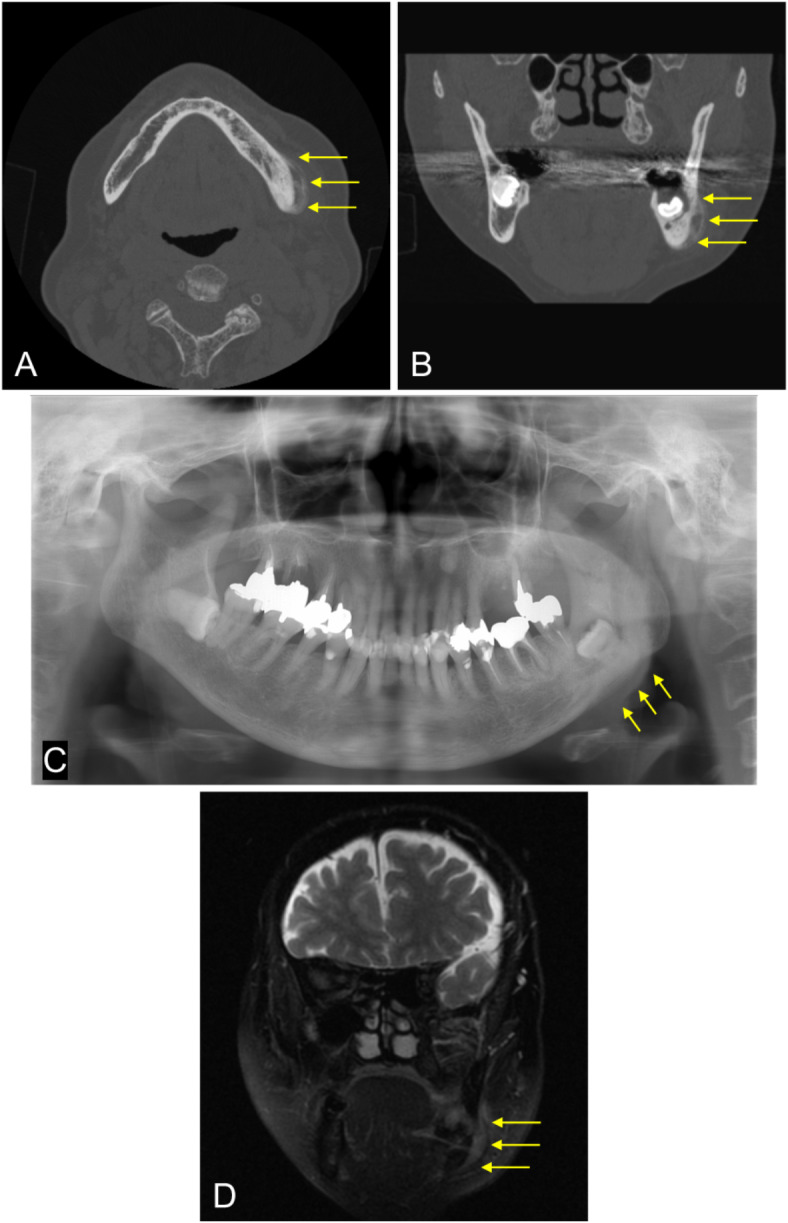
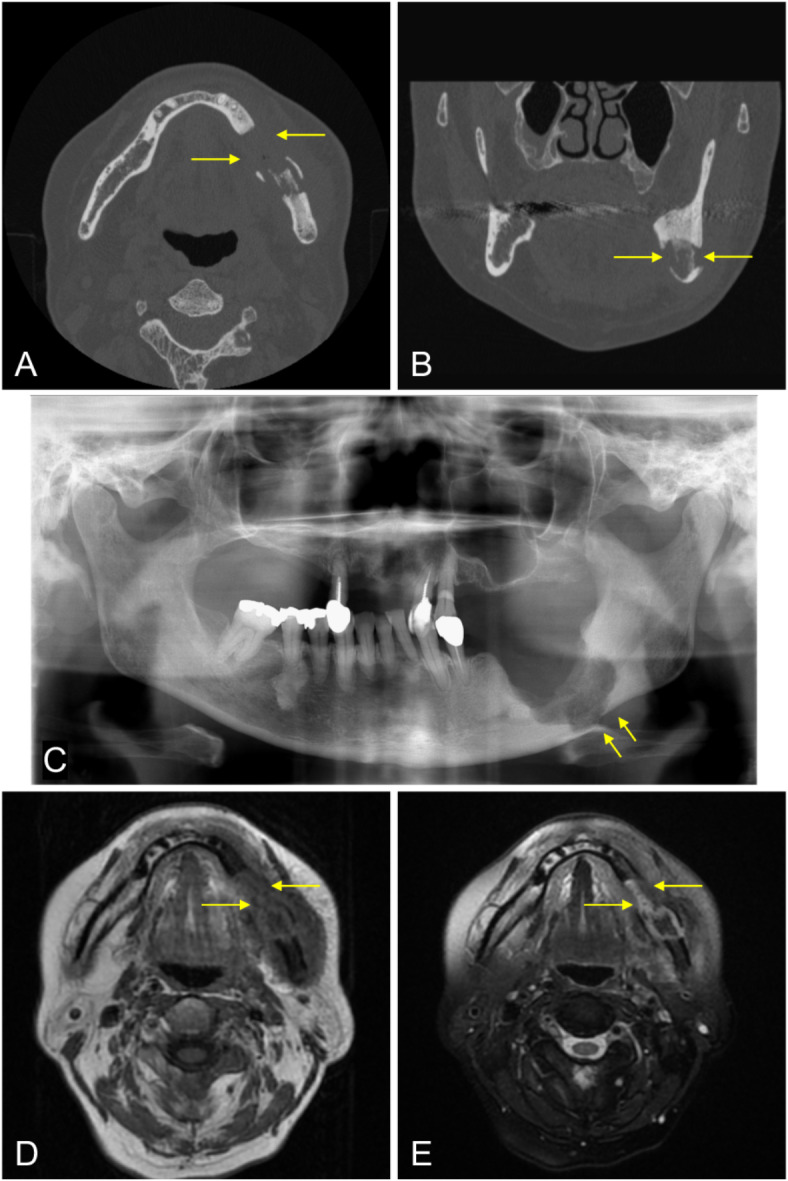
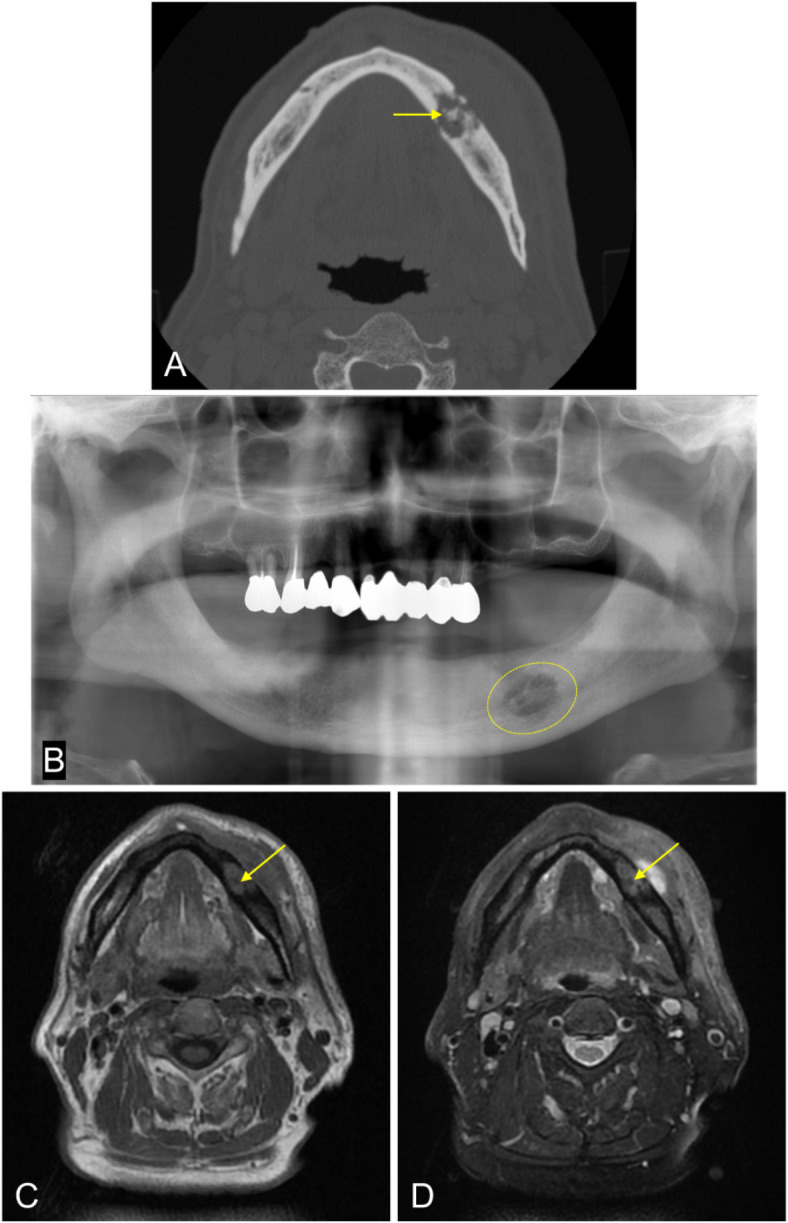
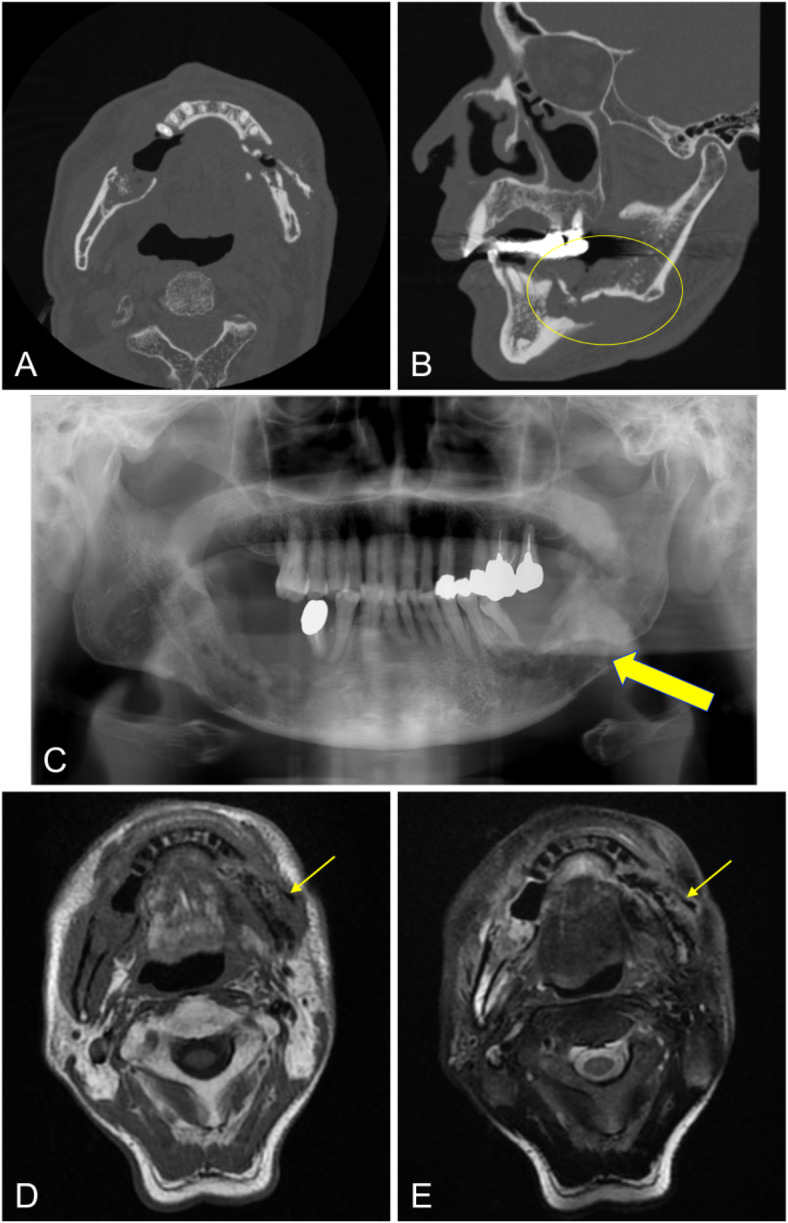
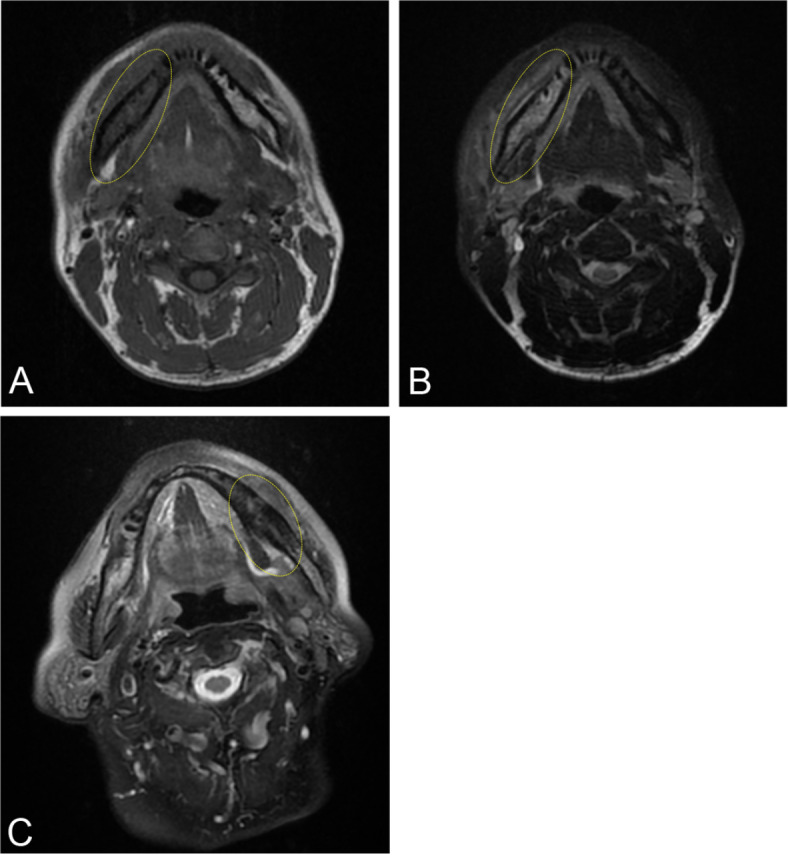
To examine the CT-imaging features of subjects with bacterial osteomyelitis (OM), osteoradionecrosis (ORN), and medication-related osteonecrosis of the jaw (MRONJ) with histopathological confirmation, and to examine the diagnostic efficacy of panoramic radiography and MRI in detecting these disease features. 150 cases with preoperative CT data were selected: 61 bacterial OM, 19 ORN, and 70 MRONJ. 143 cases underwent panoramic X-ray examination, and 47 underwent MRI. The assessment criteria for imaging findings included: (1) bone resorption, (2) osteosclerosis, (3) clarity of the mandibular canal, (4) periosteal reactions, (5) cortical bone perforation, (6) sequestrum, and (7) pathological fractures. CT was considered the gold standard for assessing these features. Compared with CT, all panoramic radiographs were detectable for diagnostic features of the disease. Bone resorption was detected in 123 cases (sensitivity 91.1%), and osteosclerosis was detected in 131 cases (sensitivity 98.5%). With panoramic radiography, most changes to clarity of the mandibular canal and pathological fractures were detected (sensitivities of 87.8% and 68.8%, respectively). However, the sensitivities for detection of periosteal reactions, cortical bone perforation and sequestration were low (19.6%, 17.8% and 19.4%, respectively). Sensitivity of MRI for detecting periosteal reactions, cortical bone perforation, sequestration, and pathological fractures (27.3%, 73.5%, 35.7%, and 60.0%, respectively) was equivalent or superior to panoramic imaging. MR-specific characteristics of bone marrow edema were depicted on almost all examinations. Panoramic radiography may be adequate for identifying bone resorption and osteosclerosis. However, MRI provides more value than panoramic radiography in detecting periosteal reactions, cortical bone perforation, sequestration, and bone marrow edema.
Keywords: CT; MRI; Osteomyelitis; Panoramic radiography.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
-
- Schmitt, S. K. Osteomyelitis. Infect. Dis. Clin. North. Am.31, 325–338 (2017). - PubMed
-
- Krakowiak, P. A. Alveolar osteitis and osteomyelitis of the jaws. Oral Maxillofac. Surg. Clin. North. Am.23, 401–413 (2011). - PubMed
-
- Schuknecht, B. & Valavanis, A. Osteomyelitis of the mandible. Neuroimaging Clin. N. Am.13, 605–618 (2003). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
