

Early-life gut microbiome associates with positive vaccine take and shedding in neonatal schedule of the human neonatal rotavirus vaccine RV3-BB
- PMID: 40210877
- PMCID: PMC11986061
- DOI: 10.1038/s41467-025-58632-6
Early-life gut microbiome associates with positive vaccine take and shedding in neonatal schedule of the human neonatal rotavirus vaccine RV3-BB
Abstract
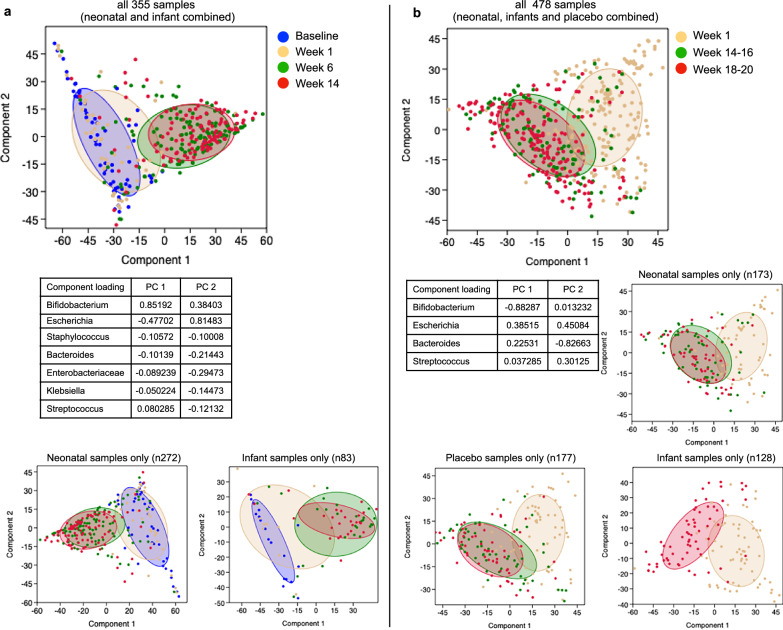
Rotavirus vaccines are less effective in high mortality regions. A rotavirus vaccine administered at birth may overcome challenges to vaccine uptake posed by a complex gut microbiome. We investigated the association between the microbiome and vaccine responses following RV3-BB vaccine (G3P[6]) administered in a neonatal schedule (dose 1: 0-5 days), or infant schedule (dose 1: 6-8 weeks) in Indonesia (Phase 2b efficacy study) (n = 478 samples/193 infants) (ACTRN12612001282875) and in Malawi (Immunigenicity study) (n = 355 samples/186 infants) (NCT03483116). Vaccine responses assessed using anti-rotavirus IgA seroconversion (IgA), stool shedding of vaccine virus and vaccine take (IgA seroconversion and/or shedding). Here we report, high alpha diversity, beta diversity differences and high abundance of Bacteroides is associated with positive vaccine take and shedding following RV3-BB administered in the neonatal schedule, but not with IgA seroconversion, or in the infant schedule. Higher alpha diversity was associated with shedding after three doses of RV3-BB in the neonatal schedule compared to non-shedders, or the placebo group. High abundance of Streptococcus and Staphylococcus is associated with no shedding in the neonatal schedule group. RV3-BB vaccine administered in a neonatal schedule modulates the early microbiome environment and presents a window of opportunity to optimise protection from rotavirus disease.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: MCRI holds the patent for the RV3-BB vaccine; J.W., J.E.B., A.H., C.M.D., E.L., D.S.O., R.B., D.P., N.B.D., K.B., J.P.B., E.W., and F.J. are employees of MCRI. C.M.D. has served on advisory boards for GSK (2019, 2021), with all payments directed to an administrative fund held by MCRI. N.C. is a National Institute for Health and Care Research (NIHR) Senior Investigator (NIHR203756). N.C., D.W., A.T., and K.C.J. are affiliated to the NIHR Global Health Research Group on Gastrointestinal Infections at the University of Liverpool; and to the NIHR Health Protection Research Unit in Gastrointestinal Infections at the University of Liverpool, a partnership with the UK Health Security Agency in collaboration with the University of Warwick. The views expressed are those of the author(s) and not necessarily those of the NIHR, the Department of Health and Social Care, the UK government or the UK Health Security Agency. All the remaining authors do not have competing interests.
Figures







References
-
- International Vaccine Access Center (IVAC). Vaccine Information Management System (VIMS) global rotavirus vaccine access report. Baltimore: John Hopkins Bloomberg School of Public Health. https://view-hub.org/vaccine/rota (2024).
-
- Armah, G. E. et al. Efficacy of pentavalent rotavirus vaccine against severe rotavirus gastroenteritis in infants in developing countries in sub-Saharan Africa: a randomised, double-blind, placebo-controlled trial. Lancet376, 606–614 (2010). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 1164384/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1058454/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1164384/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1111055/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1058454/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1164384/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1111055/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1058454/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1164384/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1111055/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1054584/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1164384/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1111055/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1058454/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- 1111055/Bill and Melinda Gates Institute for Population and Reproductive Health (Gates Institute)
- 1012425/Department of Health | National Health and Medical Research Council (NHMRC)
- 1012425/Department of Health | National Health and Medical Research Council (NHMRC)
- 1012425/Department of Health | National Health and Medical Research Council (NHMRC)
- 1012425/Department of Health | National Health and Medical Research Council (NHMRC)
- 1012425/Department of Health | National Health and Medical Research Council (NHMRC)
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
