

Transdiagnostic types of formal thought disorder and their association with gray matter brain structure: a model-based cluster analytic approach
- PMID: 40210978
- PMCID: PMC12339403
- DOI: 10.1038/s41380-025-03009-w
Transdiagnostic types of formal thought disorder and their association with gray matter brain structure: a model-based cluster analytic approach
Abstract
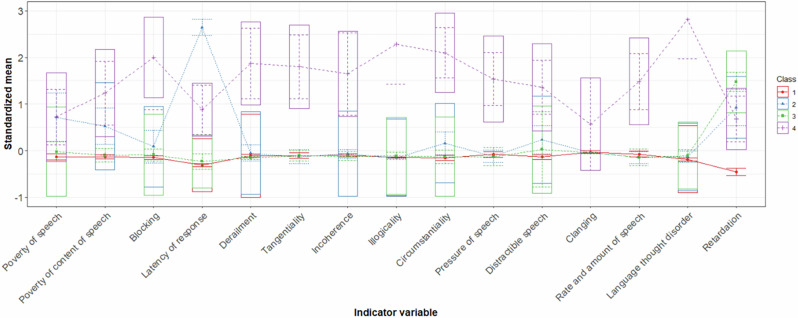
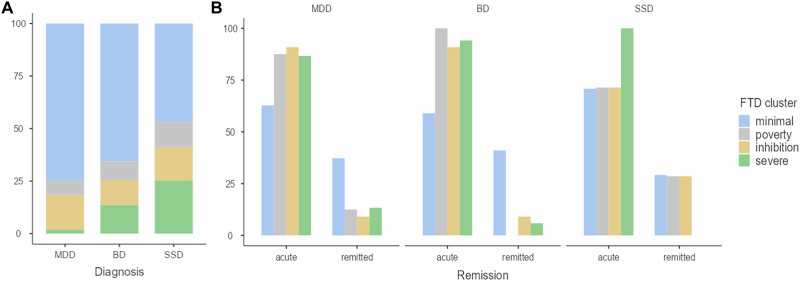
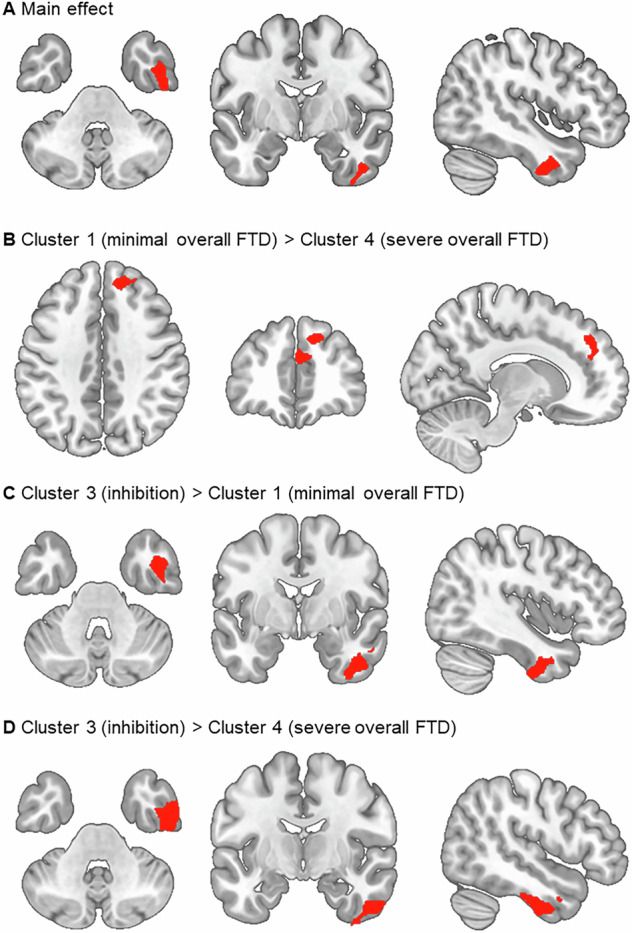
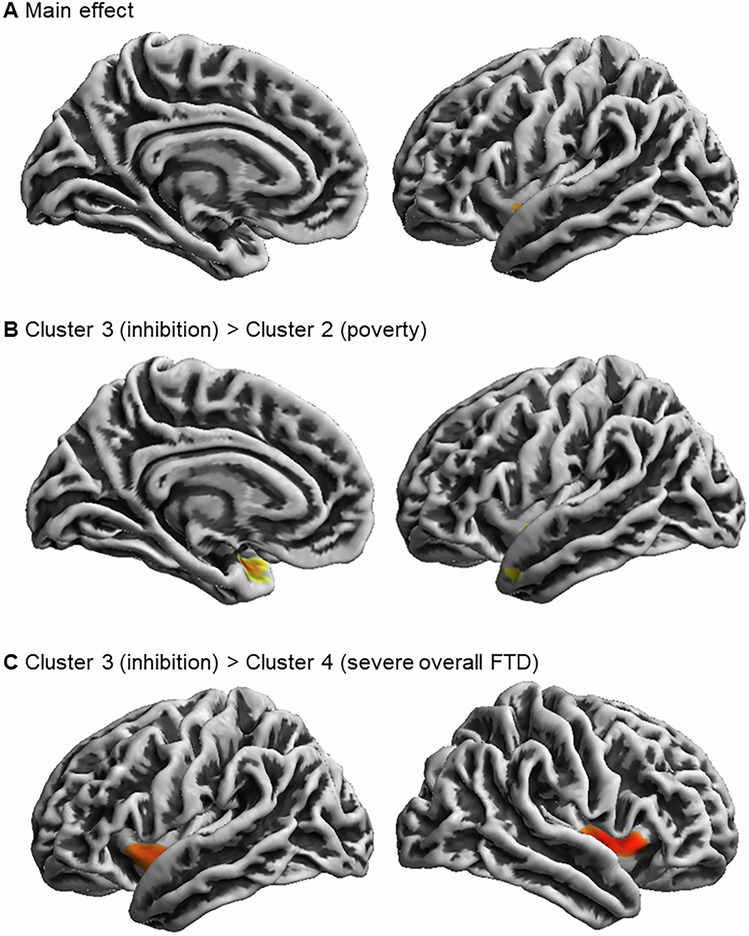
Formal thought disorder (FTD) is a complex syndrome affecting language and thought processes in psychotic and affective disorders. Clustering (i.e., identification of data-driven clinical subtypes) establishes latent (sub-) structures into psychopathological syndromes. A latent profile analysis (LPA) of FTD symptoms was conducted in 1 032 patients diagnosed with Schizophrenia-Spectrum-Disorders (n = 107), Major Depressive (n = 800), and Bipolar Disorder (n = 125). Clusters were compared for cognition and psychopathology. Associations with gray matter volume (GMV) and cortical surface (gyrification, cortical complexity, sucal depth) were explored using T1-weighted MRI data, analyzed with CAT12. Robustness-analyses in an age- and sex-matched subsample (n = 321) with the same n for each diagnosis (n = 107) were applied. LPA revealed 4 transdiagnostic clusters: minimal FTD, poverty, inhibition, severe FTD that remained stable in an age- and sex-matched subsample and in each diagnosis separately. Patients exhibiting severe FTD compared to minimal FTD showed GMV reductions in the right superior and middle frontal gyri. Inhibition showed a GMV reduction in the right inferior and middle temporal gyri, and fusiform gyrus compared with minimal and severe FTD. Sulcal depth was reduced around the left insula, superior temporal sulcus and temporal pole in the poverty cluster, and in the bilateral insula in the severe cluster, both compared to the inhibition cluster. No results for cortical thickness, gyrification, and complexity were found. Results from the total sample could be replicated in the matched subsample. Our results unravel the clinical heterogeneity of FTD psychopathology across affective and psychotic disorders. Associations of FTD clusters with neuroanatomical substrates imply language-related brain structures being involved in thought and language impairment.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Biomedical financial interests or potential conflicts of interest: Tilo Kircher received unrestricted educational grants from Servier, Janssen, Recordati, Aristo, Otsuka, and neuraxpharm. All other authors declare no conflict of interest.
Figures
Similar articles
-
Characteristics of Cerebral Cortical Structural Alterations in Female Patients with Systemic Lupus Erythematosus Without Major Neuropsychiatric Manifestations Accompanied by Anxiety and Depression.J Integr Neurosci. 2025 Jun 24;24(6):36382. doi: 10.31083/JIN36382. J Integr Neurosci. 2025. PMID: 40613368
-
Examining the relationship between gray matter volume and a continuous measure of bipolarity in unmedicated unipolar and bipolar depression.J Affect Disord. 2021 Feb 1;280(Pt A):105-113. doi: 10.1016/j.jad.2020.10.071. Epub 2020 Nov 5. J Affect Disord. 2021. PMID: 33207282 Free PMC article.
-
Morphological analysis and functional connectivity of the insular in patients with dysphagia after cerebral infarction based on resting-state fMRI.BMC Neurol. 2025 Jul 30;25(1):307. doi: 10.1186/s12883-025-04322-1. BMC Neurol. 2025. PMID: 40739609 Free PMC article.
-
Voxel-based morphometry for separation of schizophrenia from other types of psychosis in first episode psychosis.Cochrane Database Syst Rev. 2015 Aug 7;2015(8):CD011021. doi: 10.1002/14651858.CD011021.pub2. Cochrane Database Syst Rev. 2015. PMID: 26252640 Free PMC article.
-
Factors that influence participation in physical activity for people with bipolar disorder: a synthesis of qualitative evidence.Cochrane Database Syst Rev. 2024 Jun 4;6(6):CD013557. doi: 10.1002/14651858.CD013557.pub2. Cochrane Database Syst Rev. 2024. PMID: 38837220 Free PMC article. Review.
References
-
- Palaniyappan L. Dissecting the neurobiology of linguistic disorganisation and impoverishment in schizophrenia. Semin Cell Dev Biol. 2022;129:47–60. - PubMed
-
- Yalincetin B, Bora E, Binbay T, Ulas H, Akdede BB, Alptekin K. Formal thought disorder in schizophrenia and bipolar disorder: a systematic review and meta-analysis. Schizophr Res. 2017;185:2–8. - PubMed
-
- Kircher T, Bröhl H, Meier F, Engelen J. Formal thought disorders: from phenomenology to neurobiology. Lancet Psychiatry. 2018;5:515–26. - PubMed
-
- Hinzen W, Palaniyappan L. The ‘L-factor’: language as a transdiagnostic dimension in psychopathology. Prog Neuropsychopharmacol Biol Psychiatry. 2024;131:110952. - PubMed
MeSH terms
Grants and funding
- STE3301/1-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- HA 7070/2-2/Deutsche Forschungsgemeinschaft (German Research Foundation)
- JA 1890/7-1, JA 1890/7-2/Deutsche Forschungsgemeinschaft (German Research Foundation)
- KR 3822/5-1, KR 3822/7-2/Deutsche Forschungsgemeinschaft (German Research Foundation)
- NE 2254/1-2, NE 2254/2-1, NE 2254/3-1, NE 2254/4-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
LinkOut - more resources
Full Text Sources
Miscellaneous
