

Novel insights into myocardial fibrosis in patients with new onset ST-elevation myocardial infarction following percutaneous coronary intervention through enhanced cardiac magnetic resonance imaging: a prospective cohort study
- PMID: 40211110
- PMCID: PMC11983772
- DOI: 10.1186/s12872-025-04719-3
Novel insights into myocardial fibrosis in patients with new onset ST-elevation myocardial infarction following percutaneous coronary intervention through enhanced cardiac magnetic resonance imaging: a prospective cohort study
Abstract
Background: Myocardial fibrosis is a prevalent pathological hallmark of a diverse range of chronic and acute cardiovascular disorders. However, the relevant literature currently provides limited evidence regarding the determinants of myocardial fibrosis severity in patients with new-onset ST-elevation myocardial infarction (STEMI) following successful emergent percutaneous coronary intervention (PCI) utilizing contrast-enhanced cardiac magnetic resonance imaging (CE-CMR).
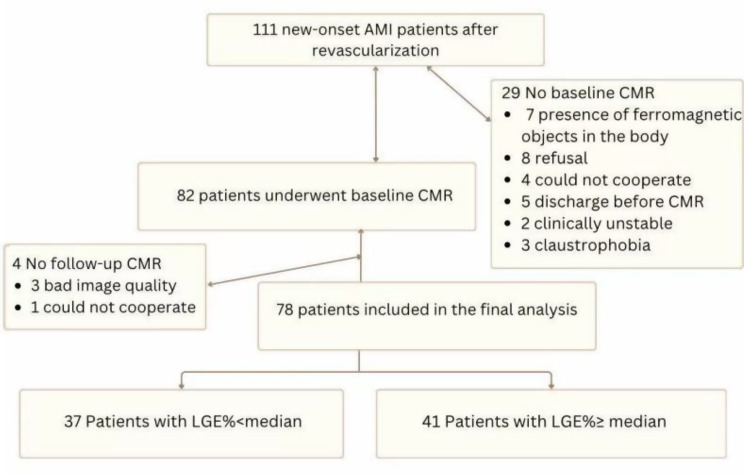
Methods: We prospectively enrolled a cohort of 78 patients who presented with new-onset ST-segment elevation myocardial infarction and who underwent successful emergent PCI within 12 h from the onset of symptoms. Late gadolinium-enhanced LGE (LGE) was quantified via CE-CMR, and patients were categorized into two groups on the basis of the median LGE value.
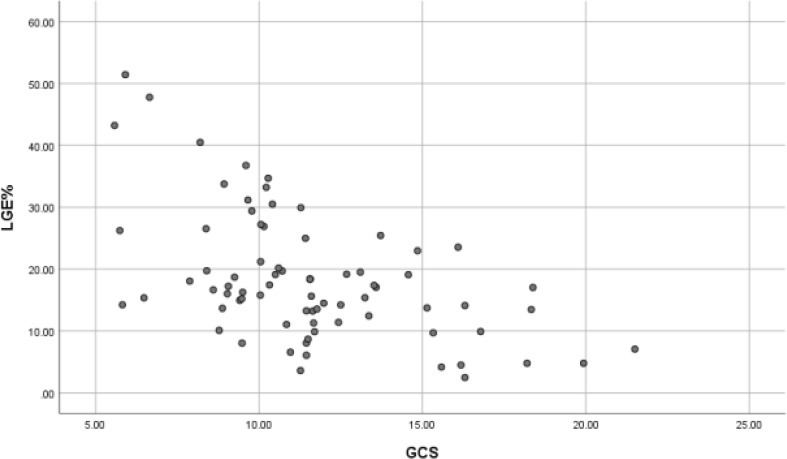
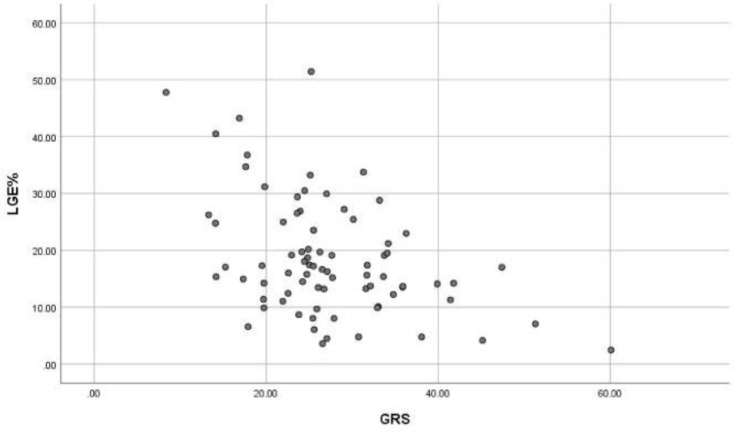
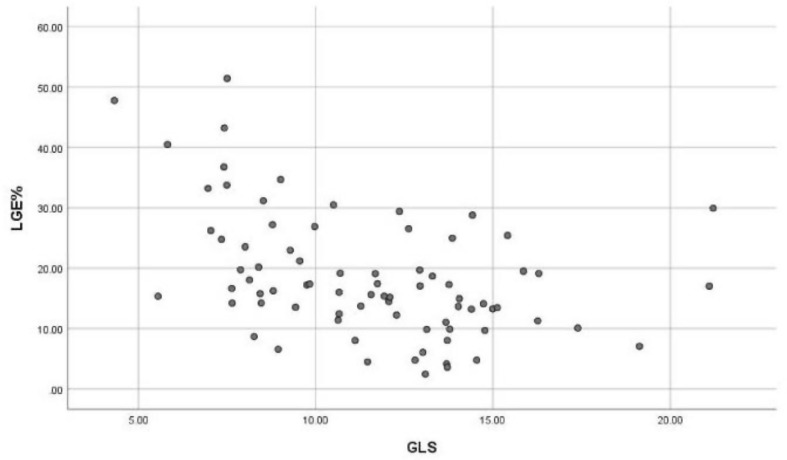
Results: The median LGE was 16% (IQR 12 to 24). Compared with patients with LGE below the median (n = 37), those with LGE above the median (n = 41) presented significantly reduced left ventricular global radial strain(GRS), global circumferential strain(GCS), and global longitudinal strain(GLS) (all p < 0.05). The infarcted radial segment (IRS), infarcted circumferential segment (ICS) and infarcted longitudinal segment (ILS) were significantly reduced in patients with greater LGE (all p < 0.05). The occurrence rates of microvascular obstruction (MVO) (p < 0.001) and wall motion abnormality (WMA) (p < 0.01) were significantly greater in patients with a greater extent of LGE, despite successful reperfusion therapy. LGE exhibited a moderate negative correlation with the global circumferential segment (r=-0.547, p < 0.001) and a weak negative correlation with both the global radial segment and the global longitudinal segment (r=-0.434, p < 0.001; r=-0.437, p < 0.001). In the multivariable linear regression analysis model, the Gensini score (β = 0.258; p < 0.01), LVEF% (β=-0.269; p < 0.05), MVO (β = 0.343; p < 0.001) and GRS (β = 0.227; p < 0.05) emerged as robust predictors of myocardial fibrosis.
Conclusion: The present study revealed a correlation of cardiac pathological structure, microcirculation, and myocardial fibrosis in the context of acute myocardial infarction. Therefore, this study provides theoretical evidence from a pathological perspective regarding the progression of myocardial fibrosis in patients with new-onset STEMI following successful PCI.
Trial registration: The trial was registered in the Chinese Clinical Trial Registry (ChiCTR2400080282; January 25th, 2024).
Keywords: Acute ST-segment elevation myocardial infarction; Cardiac magnetic resonance; Late gadolinium enhancement; Myocardial fibrosis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This study was approved by the Ethics Committee of the First Affiliated Hospital of Bengbu Medical University ([2023]KY046). Informed consent: Written informed consent for publication of their clinical details and/or clinical images was obtained from the patients. A copy of the consent form is available for review by the editor of this journal. Guarantor: The scientific guarantor of this publication is Hongju Wang. Statistics and biometry: Miaonan Li and Jun Wang kindly provided statistical advice for this manuscript. No complex statistical methods were necessary for this study. Study subject or cohort overlap: None. Methodology: Methodology: Prospective. prognostic study/observational. Performed at one institution. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bhatt DL. Lopes RD,Harrington ra.diagnosis and treatment of acute coronary syndromes. Rev [J] JAMA 2022,7:662–75. - PubMed
-
- Arbab-Zadeh A. Fuster V.From detecting the vulnerable plaque to managing the vulnerable patient: JACC State-of-the-Art review. [J] J Am Coll Cardiol. 2019;12:1582–93. - PubMed
-
- Tang L, Wu M, Xu Y, et al. Multimodal data-driven prognostic model for predicting new-onset ST-elevation myocardial infarction following emergency percutaneous coronary intervention[. J] Inflamm Res. 2023;9:1799–809. - PubMed
MeSH terms
Substances
Grants and funding
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 2022AH051477/The Key Project of Natural Science Research of the Anhui Provincial Department of Education
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 202304295107020086/Clinical research transformation project of Anhui Province
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 2022050/The First Affiliated Hospital of Bengbu Medical University
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
- 51201317/512 Talent Cultivation Program
LinkOut - more resources
Full Text Sources
Miscellaneous
