

Effect of abduction brace wearing angle on clinical outcomes after arthroscopic repair of large repairable rotator cuff: a retrospective study
- PMID: 40211329
- PMCID: PMC11983865
- DOI: 10.1186/s13018-025-05786-0
Effect of abduction brace wearing angle on clinical outcomes after arthroscopic repair of large repairable rotator cuff: a retrospective study
Abstract
Background: Rotator cuff tears affect approximately 20% of the population and are usually repaired arthroscopically. The clinical outcomes of these repairs are influenced by multiple factors, including patient characteristics, surgical technique, and postoperative management. Postoperative shoulder posture, particularly the degree of abduction, plays an important role in repair site tension and tendon-bone healing. This study aimed to evaluate the clinical outcomes and repair integrity of patients undergoing arthroscopic repair of large rotator cuff tears using a 30° and 45° abduction brace.
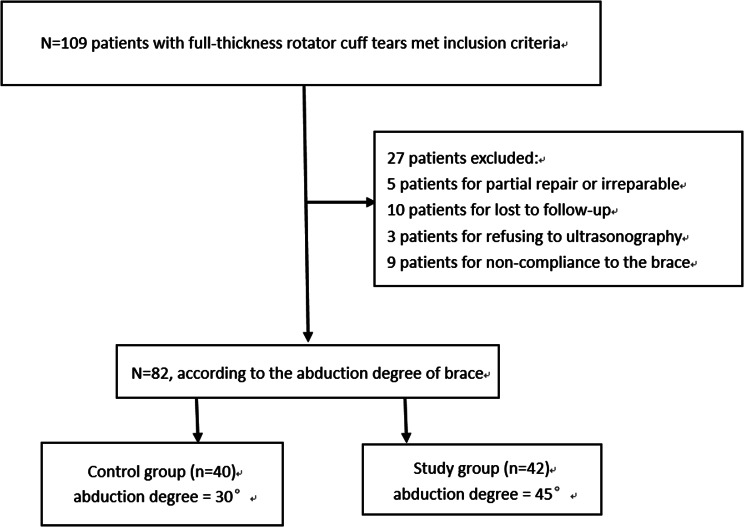
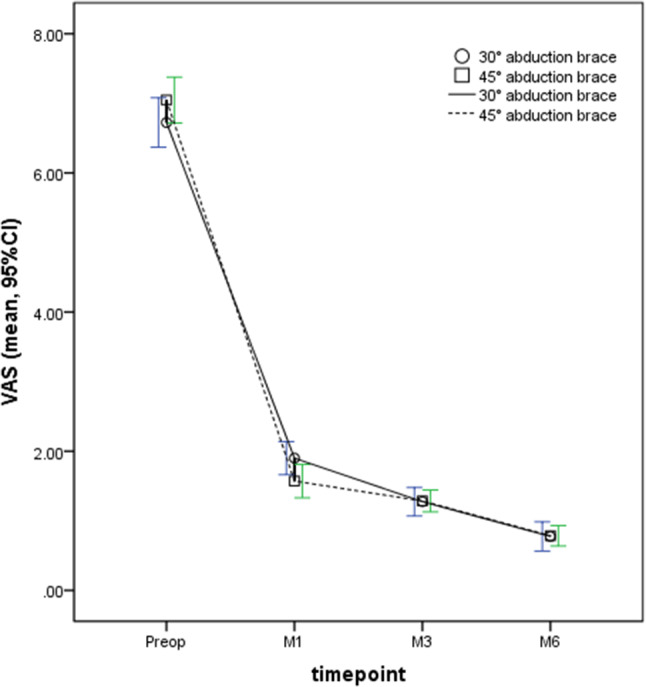
Methods: A total of 82 patients with symptomatic full-thickness rotator cuff tears were included in this study. The control group included 40 patients using a 30° brace, and the study group included 42 patients using a 45° abduction brace. Visual analogue scales (VAS) and humerohumeral range of motion were obtained before surgery and at 1 month (M1), 3 months (M3), and 6 months (M6) after surgery. Shoulder function scores (including Constant-Murley (CMS), University of California, Los Angeles (UCLA), and American Shoulder and Elbow Surgeons (ASES) scores) and retear rates were assessed at final follow-up (24 months).
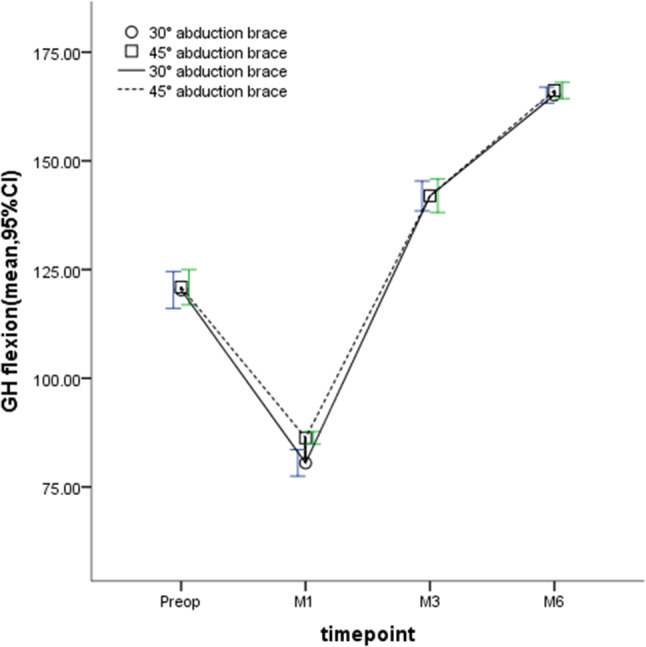
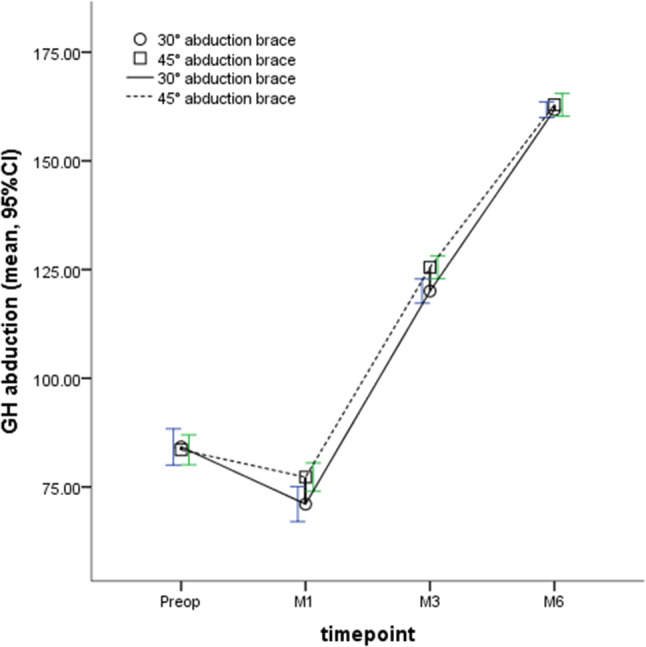
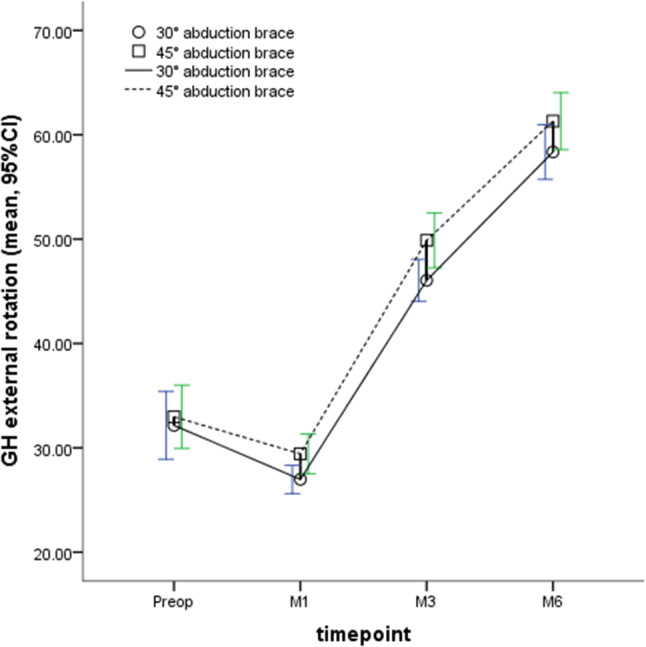
Results: Early passive ROM (flexion at 1 month, abduction at 1 and 3 months, external rotation at 1 and 3 months) was significantly better in the study group (45° abduction brace, P < 0.05). At 24 months, there were no significant differences in shoulder range of motion, function scores, and retear rates between the two groups (P > 0.05). Of note, in subgroup analysis, the retear rate was lower with a 45° brace than with a 30° brace under moderate to severe repair tension (16.67% vs. 44.44%, P < 0.05).
Conclusions: These results suggest that immobilization with a 45° brace rather than a 30° abduction brace after arthroscopic repair of large rotator cuff tears results in better passive range of motion during early follow-up, particularly with lower retear rates at moderate to severe repair strains.
Keywords: 45/30 degrees; Arthroscopy; Brace; Rotator cuff; Shoulder.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Clinical outcomes of medialized single-row repair with fascia lata graft augmentation for large and massive rotator cuff tears.J Shoulder Elbow Surg. 2024 Mar;33(3):e153-e161. doi: 10.1016/j.jse.2023.07.020. Epub 2023 Aug 22. J Shoulder Elbow Surg. 2024. PMID: 37619927
-
Anchorless Arthroscopic Transosseous and Anchored Arthroscopic Transosseous Equivalent Rotator Cuff Repair Show No Differences in Structural Integrity or Patient-reported Outcomes in a Matched Cohort.Clin Orthop Relat Res. 2020 Jun;478(6):1295-1303. doi: 10.1097/CORR.0000000000001151. Clin Orthop Relat Res. 2020. PMID: 32039957 Free PMC article.
-
Is early passive motion exercise necessary after arthroscopic rotator cuff repair?Am J Sports Med. 2012 Apr;40(4):815-21. doi: 10.1177/0363546511434287. Epub 2012 Jan 27. Am J Sports Med. 2012. PMID: 22287641 Clinical Trial.
-
Effects of early exercise and immobilization after arthroscopic rotator cuff repair surgery: a systematic review and meta-analysis of randomized controlled trials.BMC Musculoskelet Disord. 2025 Mar 13;26(1):254. doi: 10.1186/s12891-025-08500-7. BMC Musculoskelet Disord. 2025. PMID: 40082920 Free PMC article.
-
Early versus delayed mobilization for arthroscopic rotator cuff repair (small to large sized tear): a meta-analysis of randomized controlled trials.BMC Musculoskelet Disord. 2023 Dec 4;24(1):938. doi: 10.1186/s12891-023-07075-5. BMC Musculoskelet Disord. 2023. PMID: 38049792 Free PMC article.
References
-
- Yamamoto A, Takagishi K, Osawa T, Yanagawa T, Nakajima D, Shitara H, Kobayashi T. Prevalence and risk factors of a rotator cuff tear in the general population. J Shoulder Elb Surg. 2010;19:116–20. - PubMed
-
- Boileau P, Baqué F, Valerio L, Ahrens P, Chuinard C, Trojani C. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am. 2007;89:747–57. - PubMed
-
- Migliorini F, Maffulli N, Eschweiler J, Schenker H, Tingart M, Betsch M. Arthroscopic versus mini-open rotator cuff repair: A meta-analysis. Surgeon. 2023;21:e1–12. - PubMed
-
- Bedi A, Bishop J, Keener J, et al. Rotator cuff tears. Nat Rev Dis Primers. 2024;10:8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
