

Anatomical Importance Between Neural Structure and Bony Landmark in Neuroventral Decompression for Posterior Endoscopic Cervical Discectomy
- PMID: 40211534
- PMCID: PMC12010839
- DOI: 10.14245/ns.2448794.397
Anatomical Importance Between Neural Structure and Bony Landmark in Neuroventral Decompression for Posterior Endoscopic Cervical Discectomy
Abstract
Objective: This study aims to investigate the anatomical relationship among the nerve roots, intervertebral space, pedicles, and intradural rootlets of the cervical spine for improving operative outcomes and exploring neuroventral decompression approach in posterior endoscopic cervical discectomy (PECD).
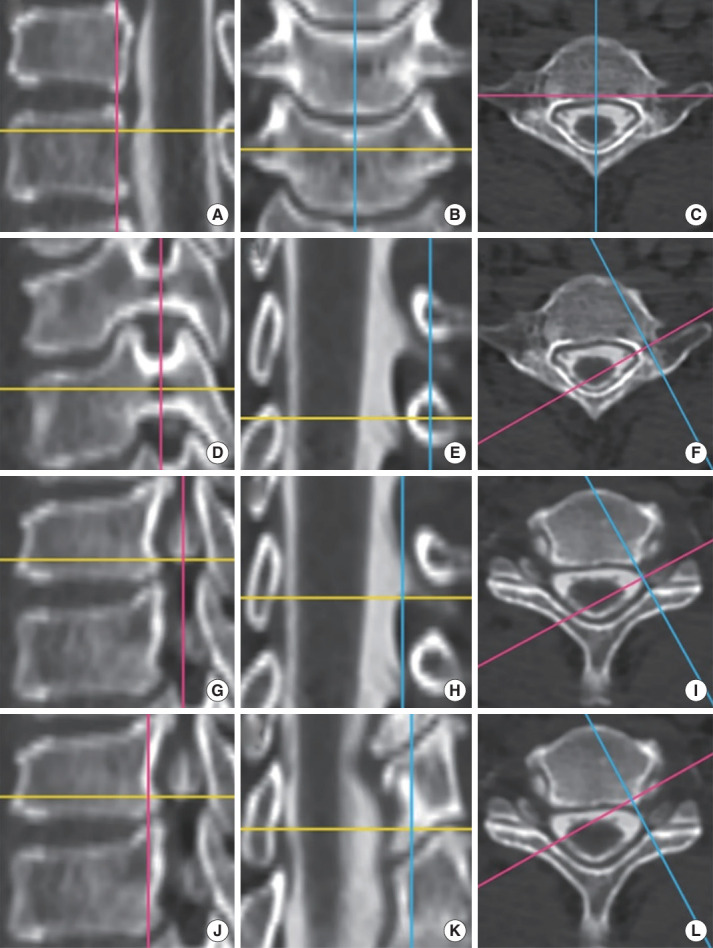
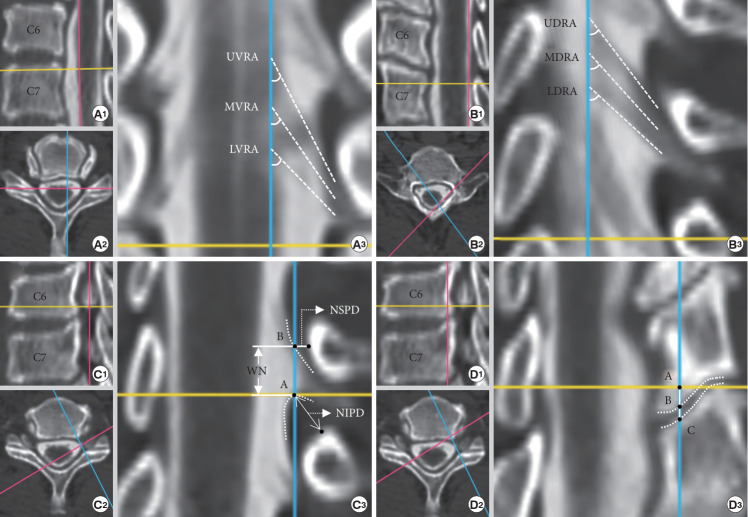
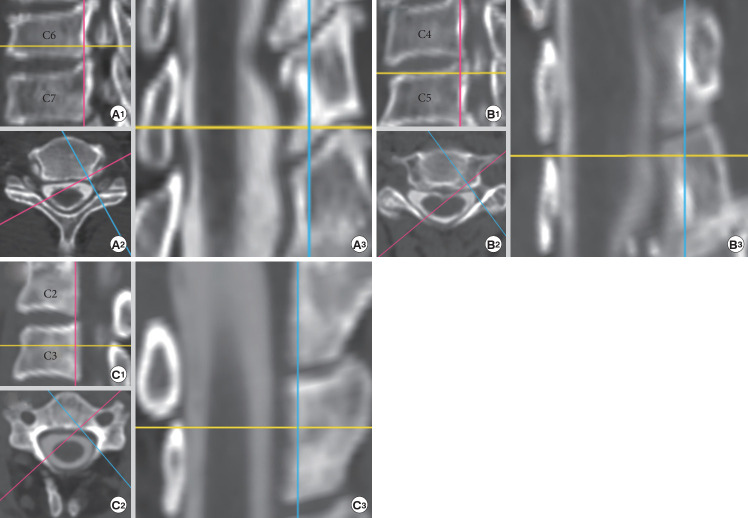
Methods: Cervical computed tomography myelography imaging data from January 2021 to May 2023 were collected, and the RadiAnt DICOM Viewer Software was employed to conduct multiplane reconstruction. The following parameters were recorded: width of nerve root (WN), nerve root-superior pedicle distance (NSPD), nerve root-inferior pedicle distance (NIPD), and the relationship between the intervertebral space and the nerve root (shoulder, anterior, and axillary). Additionally, the descending angles between the spinal cord and the ventral (VRA) and dorsal (DRA) rootlets were measured.
Results: The WN showed a gradual increase from C4 to C7, with measurements notably larger in men compared to women. The NSPD decreased gradually from the C2-3 to the C5-6 levels. However, the NIPD showed an opposite level-related change, notably larger than the NSPD at the C4-5, C5-6, and C7-T1 levels. Furthermore, significant differences in NIPD were observed between different age groups and genders. The incidence of the anterior type exhibited a gradual decrease from the C2-3 to the C5-6 levels. Conversely, the axillary type exhibited an opposite level-related change. Additionally, the VRA and DRA decreased as the level descended, with measurements significantly larger in females.
Conclusion: A prediction of the positional relationship between the intervertebral space and the nerve root is essential for the direct neuroventral decompression in PECD to avoid damaging the neural structures. The axillary route of the nerve root offers a safer and more effective pathway for performing direct neuroventral decompression compared to the shoulder approach.
Keywords: Cervical spine anatomy; Endoscopic spine surgery; Myelography; Posterior cervical discectomy.
Conflict of interest statement
The authors have nothing to disclose.
Figures
Similar articles
-
The Anatomical Relationship Between the Cervical Nerve Roots, Intervertebral Discs and Bony Cervical Landmark for Posterior Endoscopic Cervical Foraminotomy and Discectomy: A Cadaveric Study.Global Spine J. 2024 Sep;14(7):2116-2123. doi: 10.1177/21925682231217251. Epub 2023 Nov 20. Global Spine J. 2024. PMID: 37983557 Free PMC article.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Anterior transcorporeal approach of percutaneous endoscopic cervical discectomy for disc herniation at the C4-C5 levels: a technical note.Spine J. 2016 May;16(5):659-66. doi: 10.1016/j.spinee.2016.01.187. Epub 2016 Feb 2. Spine J. 2016. PMID: 26850173
-
Anatomical Evaluation of Spinal Nerve and Cervical Intervertebral Foramina in Anterior Controllable Antedisplacement and Fusion Surgery: A Cadaveric and Radiologic Study.Orthop Surg. 2022 Feb;14(2):331-340. doi: 10.1111/os.13181. Epub 2021 Dec 22. Orthop Surg. 2022. PMID: 34935286 Free PMC article.
-
Post-operative nerve injuries after cervical spine surgery.Int Orthop. 2019 Apr;43(4):791-795. doi: 10.1007/s00264-018-4257-4. Epub 2018 Nov 29. Int Orthop. 2019. PMID: 30498911 Review.
References
-
- Corey DL, Comeau D. Cervical radiculopathy. Med Clin North Am. 2014;98:791–9. xii. - PubMed
-
- Xiao CM, Yu KX, Deng R, et al. Modified K-Hole percutaneous endoscopic surgery for cervical foraminal stenosis: partial pediculectomy approach. Pain Physician. 2019;22:E407–16. - PubMed
-
- Coric D, Adamson T. Minimally invasive cervical microendoscopic laminoforaminotomy. Neurosurg Focus. 2008;25:E2 - PubMed
-
- Tong Y, Huang Z, Hu C, et al. A comparison study of posterior cervical percutaneous endoscopic ventral bony decompression and simple dorsal decompression treatment in cervical spondylotic radiculopathy caused by cervical foraminal and/or lateral spinal stenosis: a clinical retrospective study. BMC Musculoskelet Disord. 2020;21:290. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
