

Sex disparities in alcohol-associated liver disease and subtype differences in alcohol-attributable cancers in the United States
- PMID: 40211871
- PMCID: PMC12260637
- DOI: 10.3350/cmh.2025.0169
Sex disparities in alcohol-associated liver disease and subtype differences in alcohol-attributable cancers in the United States
Abstract
Background/aims: Harmful alcohol use is a substantial contributor to liver diseases, liver cancer, and extrahepatic neoplasms. Patterns of alcohol consumption have shifted over recent decades. This study evaluates trends in alcohol-associated liver disease (ALD) and alcohol-attributable cancers in the United States (US) from 2000 to 2021.
Methods: Using the methodological framework of the Global Burden of Disease Study 2021, we analyzed trends in incidence, prevalence, and mortality from ALD and alcohol-attributable cancers in the US.
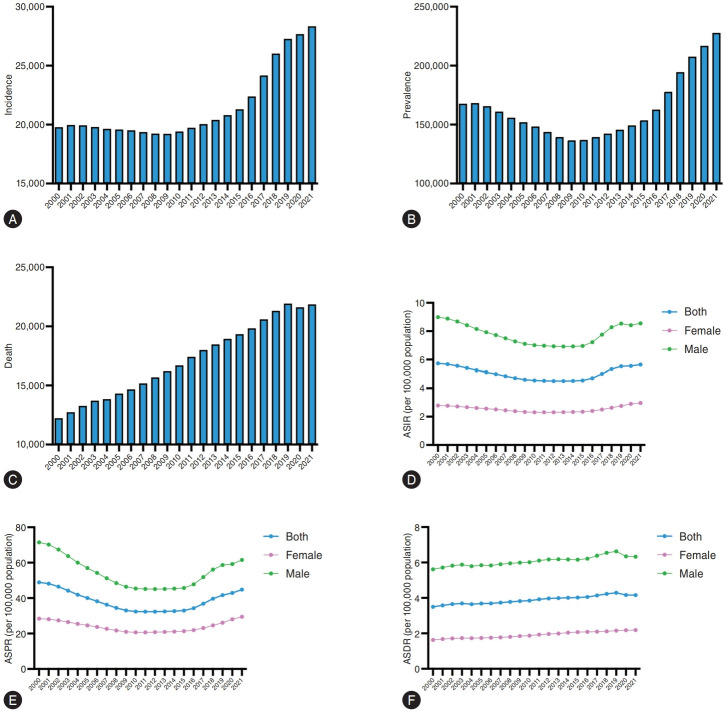
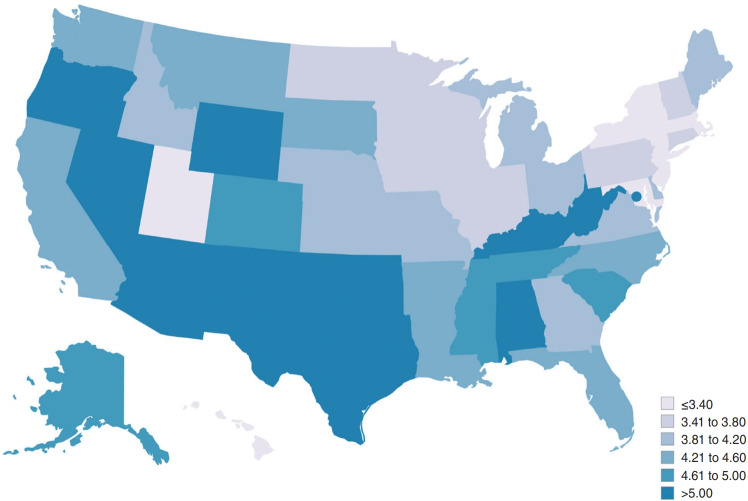
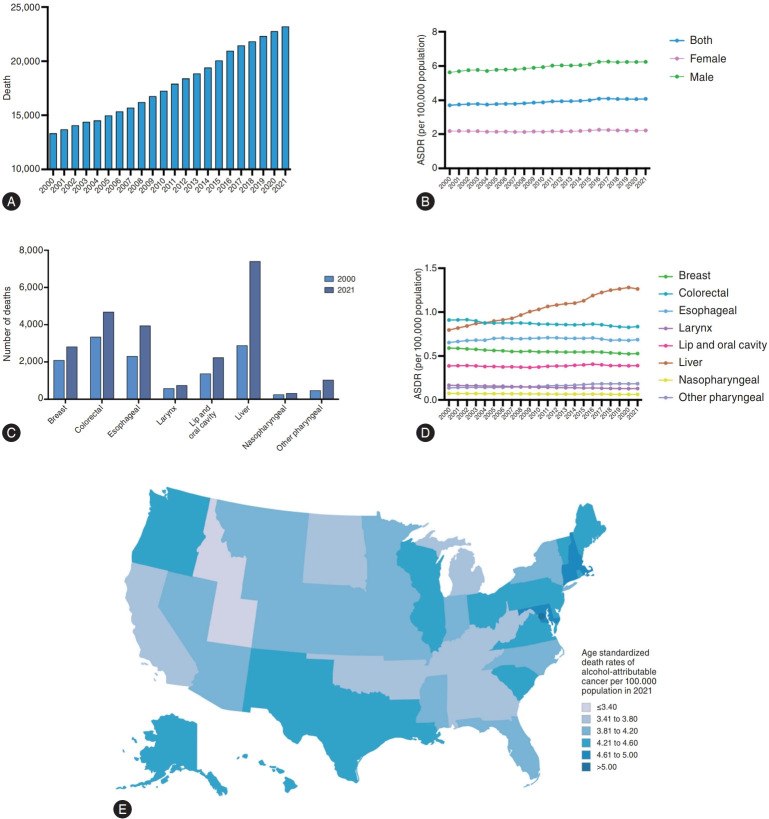
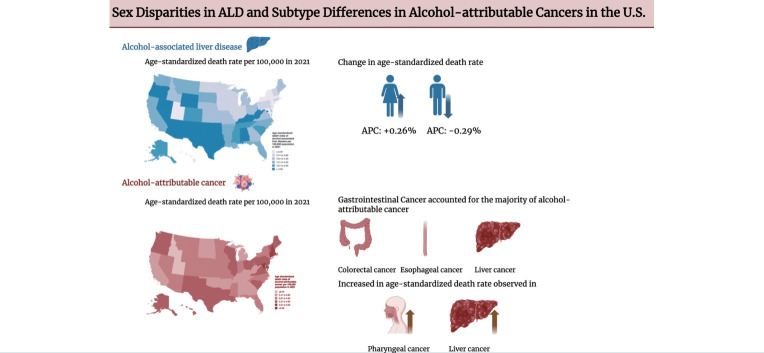
Results: In 2021, there were 28,340 new cases of ALD, 227,730 prevalent cases, and 21,860 deaths attributed to ALD in the US. From 2000 to 2021, ALD incidence, prevalence, and mortality increased by 43%, 36%, and 79%, respectively. The age-standardized incidence and death rate of ALD rose disproportionately among females compared to males. For alcohol-attributable cancers, primary liver cancer, colorectal cancer, and esophageal cancer accounted for the largest share of deaths in 2021. Age-standardized death rates increased significantly for primary liver cancer (annual percent change [APC] 2.21%, 95% confidence interval [CI] 1.70-2.73%) and other pharyngeal cancer (APC 1.35%, 95% CI 1.08-1.62%).
Conclusion: The burden of ALD is substantial and continues to rise in the US, with a particularly notable increase among females. Mortality from alcohol-attributable cancers is also increasing, mainly driven by primary liver cancer and pharyngeal cancer. However, system-wise, gastrointestinal cancer had the highest death attributable to alcohol. These findings highlight the urgent need for public health strategies to tackle ALD, primary liver cancer, and alcoholattributable extrahepatic malignancies.
Keywords: Alcohol; Chronic liver disease; Sex disparity; Steatotic liver disease.
Conflict of interest statement
Suthat Liangpunsakul has served as a consultant for Durect and Surrozen. Mazen Noureddin has been on the advisory board for 89bio, Gilead Sciences, Intercept Pharmaceuticals, Pfizer, Novo Nordisk, Blade Therapeutics, EchoSens, Fractyl Health, Terns Pharmaceuticals, Siemens, and Roche Diagnostics; has received research support from Allergan, Bristol Myers Squibb, Gilead Sciences, Galmed Pharmaceuticals, Galectin Therapeutics, Genfit, Conatus Pharmaceuticals, Enanta Pharmaceuticals, Madrigal Pharmaceuticals, Novartis, Pfizer, Shire, Viking Therapeutics and Zydus Lifesciences; and is a minor shareholder or has stocks in Anaetos, Rivus Pharmaceuticals, and Viking Therapeutics. Ju Dong Yang consults for AstraZeneca, Eisai, Exact Sciences, and Fujifilm Medical Sciences. Amit G. Singal has served as a consultant or on advisory boards for Genentech, AstraZeneca, Eisai, Exelixis, Bayer, Elevar Therapeutics, Merck, Boston Scientific, Sirtex, HistoSonics, Fujifilm Medical Sciences, Exact Sciences, Roche Diagnostics, Abbott, and Glycotest Diagnostics. Mark D. Muthiah: M.D.M has served as a consultant to Roche Diagnostics, Estella, and Gilead Sciences. He has been an advisor for Lerna Biopharma. M.D.M. has received payment from speaking at Boston Scientific, Olympus Medical, Roche Diagnostics, and Astellas Pharma. M.D.M. is supported by the Singapore Ministry of Health through the National Medical Research Council (NMRC) Office, MOH Holdings Pte Ltd under the NMRC Clinician Scientist-Individual Research Grant (MOH-001228) and NMRC Clinician Scientist Award (MOH-001631), as well as the National Research Foundation, Singapore (NRF) under the NMRC Open Fund – Large Collaborative Grant (MOH- 001325) and administered by the Singapore Ministry of Health through the NMRC Office, MOH Holdings Pte Ltd. The other authors declare no competing interests.
Figures
Similar articles
-
Trends in alcohol-associated liver disease mortality rates in American Indians and Alaskan Natives.BMC Public Health. 2025 Jun 2;25(1):2046. doi: 10.1186/s12889-025-22895-x. BMC Public Health. 2025. PMID: 40457328 Free PMC article.
-
Alcohol-Related Liver Disease, Followed by Metabolic Dysfunction-Associated Steatotic Liver Disease, Emerges as the Fastest-Growing Aetiologies for Primary Liver Cancer in the United States.Aliment Pharmacol Ther. 2025 Mar;61(6):959-970. doi: 10.1111/apt.18473. Epub 2025 Jan 5. Aliment Pharmacol Ther. 2025. PMID: 39757456
-
Trends in Hepatocellular Carcinoma Mortality Rates in the US and Projections Through 2040.JAMA Netw Open. 2024 Nov 4;7(11):e2445525. doi: 10.1001/jamanetworkopen.2024.45525. JAMA Netw Open. 2024. PMID: 39556395 Free PMC article.
-
Alcohol-associated liver disease-Global epidemiology.Hepatology. 2024 Dec 1;80(6):1307-1322. doi: 10.1097/HEP.0000000000000899. Epub 2024 Apr 19. Hepatology. 2024. PMID: 38640041 Review.
-
Epidemic characteristics of alcohol-related liver disease in Asia from 2000 to 2020: A systematic review and meta-analysis.Liver Int. 2022 Aug;42(9):1991-1998. doi: 10.1111/liv.15312. Epub 2022 May 27. Liver Int. 2022. PMID: 35593004
References
-
- Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. 2009;373:2223–2233. - PubMed
-
- Mehta G, Sheron N. No safe level of alcohol consumption - Implications for global health. J Hepatol. 2019;70:587–589. - PubMed
-
- Grant BF, Chou SP, Saha TD, Pickering RP, Kerridge BT, Ruan WJ, et al. Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV Alcohol Use Disorder in the United States, 2001-2002 to 2012-2013: Results From the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiatry. 2017;74:911–923. - PMC - PubMed
-
- Shield K, Manthey J, Rylett M, Probst C, Wettlaufer A, Parry CDH, et al. National, regional, and global burdens of disease from 2000 to 2016 attributable to alcohol use: a comparative risk assessment study. Lancet Public Health. 2020;5:e51–e61. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
