

Association between socioeconomic position and lung cancer incidence in 16 countries: a prospective cohort consortium study
- PMID: 40212049
- PMCID: PMC11985077
- DOI: 10.1016/j.eclinm.2025.103152
Association between socioeconomic position and lung cancer incidence in 16 countries: a prospective cohort consortium study
Abstract
Background: Studies have reported higher lung cancer incidence among groups with lower socioeconomic position (SEP). However, it is not known how this difference in lung cancer incidence between SEP groups varies across different geographical settings. Furthermore, most prior studies that assessed the association between SEP and lung cancer incidence were conducted without detailed adjustment for smoking. Therefore, we aimed to assess this relationship across world regions.
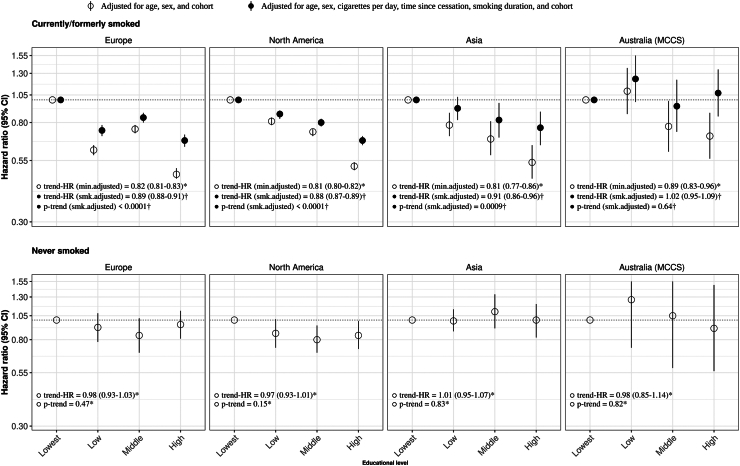
Methods: In this international prospective cohort consortium study, we used data from the Lung Cancer Cohort Consortium (LC3), which includes 20 prospective population cohorts from 16 countries in North America, Europe, Asia, and Australia. Participants were enrolled between 1985 and 2010 and followed for cancer outcomes using registry linkages and/or active follow-up. We estimated hazard ratios (HRs) for the association between educational level (our primary measure of SEP, in 4 categories) and incident lung cancer using Cox proportional hazards models separately for participants with and without a smoking history. The models were adjusted for age, sex, cohort (when multiple cohorts were included), smoking duration, cigarettes per day, and time since cessation.
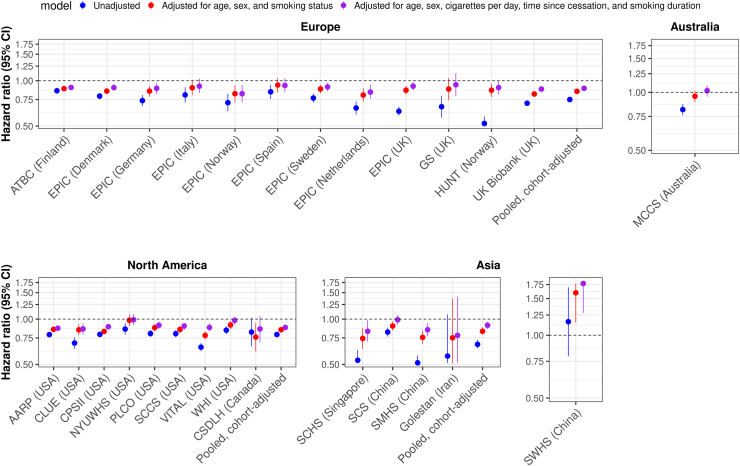
Findings: Among 2,487,511 participants, 53,830 developed lung cancer during a 13.5-year median follow-up (IQR = 6.5-15.0 years). Among participants with a smoking history, higher education was associated with decreased lung cancer incidence in nearly every cohort after detailed smoking adjustment. By world region, this association was observed in North America (HR per one-category increase in education [HRtrend] = 0.88, 95% CI = 0.87-0.89), Europe (HRtrend = 0.89, 95% CI = 0.88-0.91), and Asia (HRtrend = 0.91, 95% CI = 0.86-0.96), but not in the Australian study (HRtrend = 1.02, 95% CI = 0.95-1.09). By histological subtype, education associated most strongly with squamous cell carcinoma and more weakly with adenocarcinoma (p-heterogeneity < 0.0001). Among participants who never smoked, there was no association between education and lung cancer incidence in any cohort (all p-trend > 0.05), except the USA Southern Community Cohort Study (HRtrend = 0.75, 95% CI = 0.62-0.90).
Interpretation: Based on longitudinal data from 2.5 million participants from 16 countries, our findings suggest that higher educational attainment was associated with lower lung cancer risk among participants with a smoking history, but not among participants who never smoked. Limitations of our study include that cohort participants cannot fully represent the general populations of the geographical regions included, and education was the only measure of SEP consistently available across our consortium.
Funding: This study was supported in part by the National Cancer Institute (NCI), the Lung Cancer Research Foundation (LCRF), and the World Cancer Research Fund (WCRF).
Keywords: Geographical differences; Incidence; Lung cancer; Socioeconomic position.
© 2025 World Health Organization.
Conflict of interest statement
LE reports payments made to institution: National Cancer Institute; Lung Cancer Research Foundation; American Association of Thoracic Surgery; honoraria for giving grand rounds: UC Davis Health; honoraria for giving keynote address: Lung Cancer Health Equity Symposium; participation on a Data Safety Monitoring Board or Advisory Board (No payments): Lung Cancer Research Foundation, Bristol Myer Squibb Foundation; advisory board participation: PCORI research grant. RW reports grants from the US National Cancer Institute (R00CA256515, R01CA274716). MCA reports participation in the National Lung Cancer Roundtable (service on the Health Equity Task Group and the Lung Cancer Early Detection Implementation Strategies Task Group), and is a member of the scientific steering committee of Guardant Health. JSA reports funding from the National Institute of General Medical Sciences (NIGMS), National Cancer Institute (R01 CA282223, R01CA25925, R01CA298165), National Institute on Minority Health and Health Disparities (5R01MD017302), National Institute of Drug Abuse (1R01DA055999); consulting fees, equity, and Scientific Advisory Board chairmanship from Onovia, a start-up company working on a prescription nicotine replacement product; receipt of funds for travel expenses (no honoraria) as a speaker for the annual GTNF conferences from 2021 to 2024, the 2022 and 2024 Tobacco Science Research Conference, the 2024 Coresta annual scientific conference, and the 2021–2024 annual Food and Drug Law Institute annual scientific conferences; Board of Directors membership for the Council of Tobacco Treatment Training Programs. J-MY reports NIH/NCI grants (R01CA155809 and R01CA269223) to his institution. All other authors declare no competing interests.
Figures


Similar articles
-
Are There Sex Differences in the Association of Alcohol Consumption With the Risk of Soft Tissue Sarcoma? A Nationwide Population-based Study in Korea.Clin Orthop Relat Res. 2025 Jun 25. doi: 10.1097/CORR.0000000000003602. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40658922
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
Electronic cigarettes for smoking cessation.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD010216. doi: 10.1002/14651858.CD010216.pub7. Cochrane Database Syst Rev. 2022. Update in: Cochrane Database Syst Rev. 2024 Jan 8;1:CD010216. doi: 10.1002/14651858.CD010216.pub8. PMID: 36384212 Free PMC article. Updated.
-
Sex and gender as predictors for allograft and patient-relevant outcomes after kidney transplantation.Cochrane Database Syst Rev. 2024 Dec 19;12(12):CD014966. doi: 10.1002/14651858.CD014966.pub2. Cochrane Database Syst Rev. 2024. PMID: 39698949
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
Cited by
-
Routes to Diagnosis in Lung Cancer-Do Socio-Demographics Matter? An English Population-Based Study.Cancers (Basel). 2025 Jun 3;17(11):1874. doi: 10.3390/cancers17111874. Cancers (Basel). 2025. PMID: 40507354 Free PMC article.
References
-
- Sung H., Ferlay J., Siegel R.L., et al. Global cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. - PubMed
-
- Malhotra J., Malvezzi M., Negri E., La Vecchia C., Boffetta P. Risk factors for lung cancer worldwide. Eur Respir J. 2016;48(3):889–902. - PubMed
-
- Sidorchuk A., Agardh E.E., Aremu O., Hallqvist J., Allebeck P., Moradi T. Socioeconomic differences in lung cancer incidence: a systematic review and meta-analysis. Cancer Causes Control. 2009;20(4):459–471. - PubMed
-
- Dalton S.O., Steding-Jessen M., Jakobsen E., et al. Socioeconomic position and survival after lung cancer: influence of stage, treatment and comorbidity among Danish patients with lung cancer diagnosed in 2004-2010. Acta Oncol. 2015;54(5):797–804. - PubMed
-
- Villalba C.M.H. In: Encyclopedia of quality of life and well-being research. Michalos A.C., editor. Springer Netherlands; Dordrecht: 2014. Socioeconomic status (SES) pp. 6210–6212.
Grants and funding
LinkOut - more resources
Full Text Sources
