

Interaction and overall effects of underweight, low muscle mass, malnutrition, and inflammation on early-onset mild cognitive impairment in type 2 diabetes
- PMID: 40212567
- PMCID: PMC11983464
- DOI: 10.3389/fnagi.2025.1498478
Interaction and overall effects of underweight, low muscle mass, malnutrition, and inflammation on early-onset mild cognitive impairment in type 2 diabetes
Abstract
Introduction: This study systematically explores the overall impact and interactions of body composition and nutritional inflammatory indices on early-onset mild cognitive impairment (EOMCI) in type 2 diabetes mellitus (T2DM).
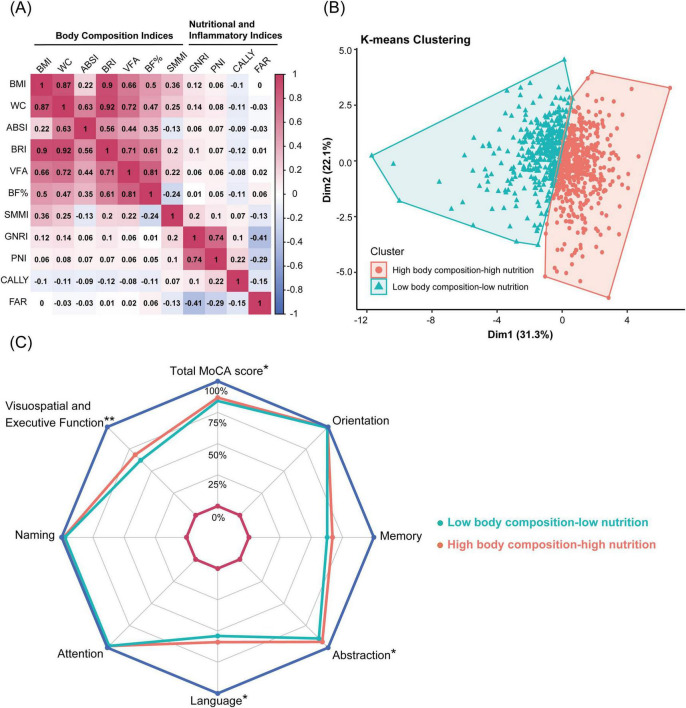
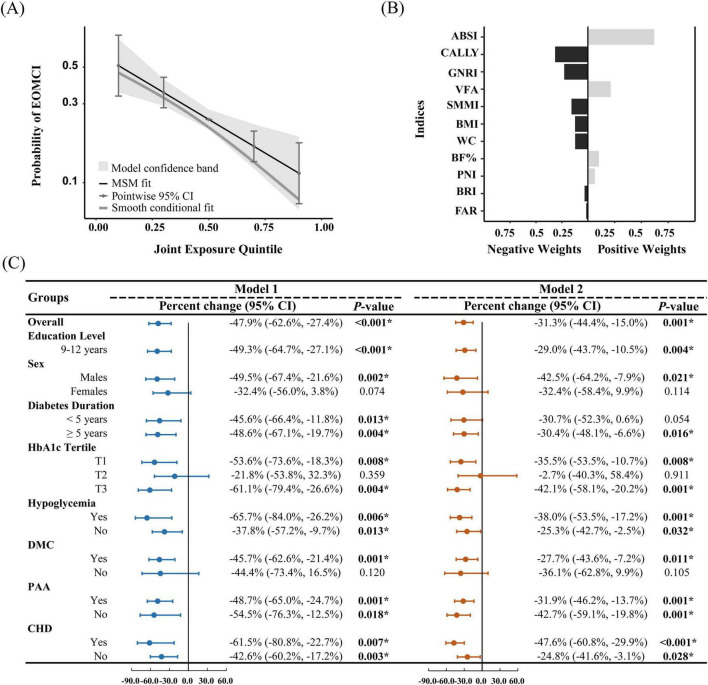
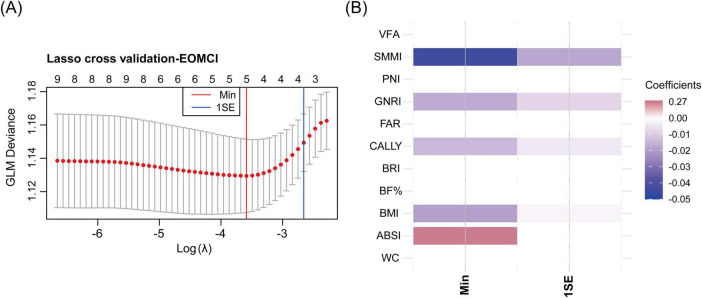
Methods: A cross-sectional study included 816 T2DM patients. Body composition indices included body mass index (BMI), waist circumference (WC), a body shape index (ABSI), body roundness index (BRI), visceral fat area (VFA), body fat percentage (BF%), and skeletal muscle mass index (SMMI). Nutritional inflammatory indices included the geriatric nutritional risk index (GNRI), prognostic nutritional index (PNI), C-reactive protein-albumin-lymphocyte index (CALLY), and fibrinogen-to-albumin ratio (FAR). K-means clustering and quantile g-computation (QGC) assessed the combined impact, with interactions evaluated by simple slope analysis.
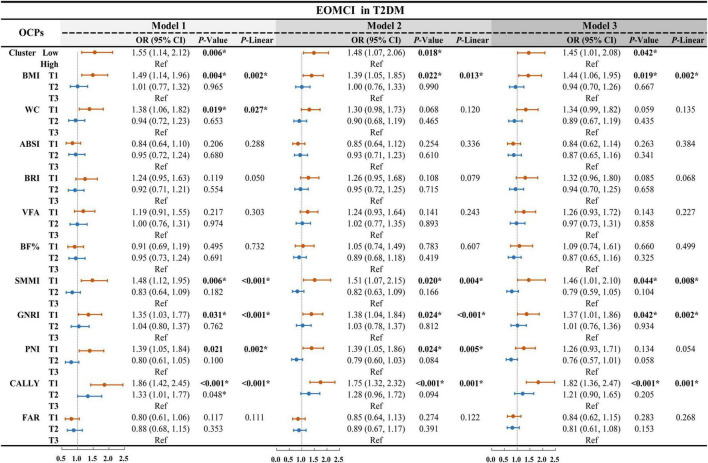
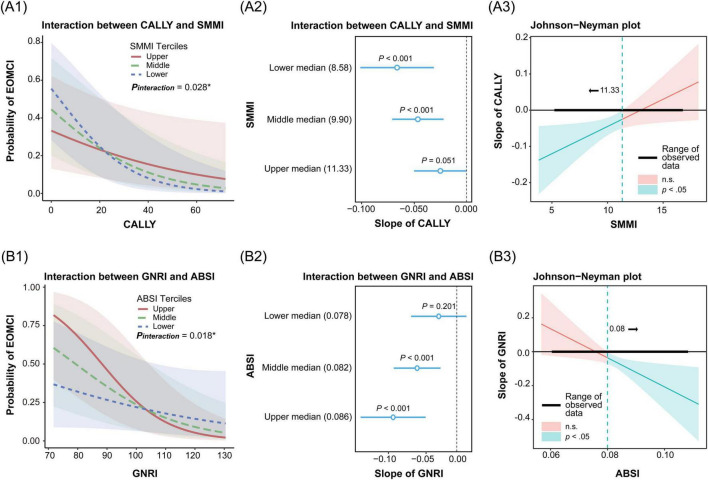
Results: K-means clustering revealed two distinct patterns: Low-pattern and High-pattern. The Low-pattern group exhibited significantly lower body composition indices (BMI 24.6 vs. 27.7 kg/m2; WC 88 vs. 99 cm; ABSI 0.081 vs. 0.084; BRI 3.89 vs. 5.02; VFA 91 vs. 112; BF% 29% vs. 31%; SMMI 9.38 vs. 10.48 kg/m2; all P < 0.001) and poorer nutritional status with higher inflammation (GNRI 97.9 vs. 104.6; PNI 47.9 vs. 53.1; CALLY index 4 vs. 5; FAR 0.082 vs. 0.072; all P < 0.05). This group had a higher prevalence of EOMCI (32% vs. 23%, P = 0.006). After adjusting for confounders, the Low-pattern group had a 1.45-fold increased risk of EOMCI (OR 1.45, 95% CI 1.01-2.08). QGC analysis demonstrated that the combined overall effect of body composition and nutritional inflammatory indices was negatively associated with EOMCI risk. A one-quintile increase in all indices was linked to a significant 31.3% reduction in EOMCI risk (95% CI -44.4%, -15.0%). Interaction analysis revealed that abdominal obesity (ABSI > 0.08), combined with malnutrition (low GNRI), significantly increased EOMCI risk (P interaction = 0.018). Similarly, low muscle mass (SMMI < 11.33 kg/m2), when combined with malnutrition and high inflammation (low CALLY index), further exacerbated EOMCI risk (P interaction = 0.028).
Discussion: The findings suggest that in T2DM patients, the interactions and overall effects of underweight, reduced muscle mass, abdominal obesity, malnutrition, and elevated inflammation are significantly associated with an increased risk of EOMCI. Integrated management of these factors is essential to mitigate EOMCI risk.
Keywords: inflammation; interaction; malnutrition; mild cognitive impairment; sarcopenia; type 2 diabetes mellitus.
Copyright © 2025 Lin, Zhai, Wu, An, Chen, Qiu, Li and Lin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A body shape index and body roundness index: two new body indices to identify diabetes mellitus among rural populations in northeast China.BMC Public Health. 2015 Aug 19;15:794. doi: 10.1186/s12889-015-2150-2. BMC Public Health. 2015. PMID: 26286520 Free PMC article.
-
Correlation Between Prognostic Nutritional Index, Glasgow Prognostic Score, and Different Obesity-Related Indices in People with Diabetes or Prediabetes.Diagnostics (Basel). 2024 Nov 26;14(23):2661. doi: 10.3390/diagnostics14232661. Diagnostics (Basel). 2024. PMID: 39682569 Free PMC article.
-
Association between visceral fat mass and arterial stiffness among community-based screening participants.Hypertens Res. 2023 Nov;46(11):2488-2496. doi: 10.1038/s41440-023-01350-7. Epub 2023 Jun 23. Hypertens Res. 2023. PMID: 37353686
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
-
Anthropometric indices and cut-off points for screening of metabolic syndrome among South African taxi drivers.Front Nutr. 2022 Aug 11;9:974749. doi: 10.3389/fnut.2022.974749. eCollection 2022. Front Nutr. 2022. PMID: 36034933 Free PMC article.
References
-
- American Medical Association. (2023). AMA Adopts New Policy Clarifying Role of BMI as a Measure in Medicine. Chicago, IL: American Medical Association.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous