

The association between cumulative adverse childhood experiences and ultra-processed food addiction is moderated by substance use disorder history among adults seeking outpatient nutrition counseling
- PMID: 40212842
- PMCID: PMC11983559
- DOI: 10.3389/fpsyt.2025.1543923
The association between cumulative adverse childhood experiences and ultra-processed food addiction is moderated by substance use disorder history among adults seeking outpatient nutrition counseling
Abstract
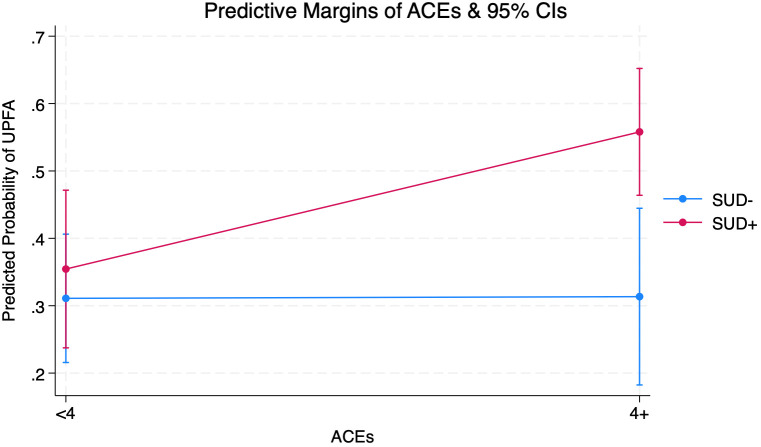
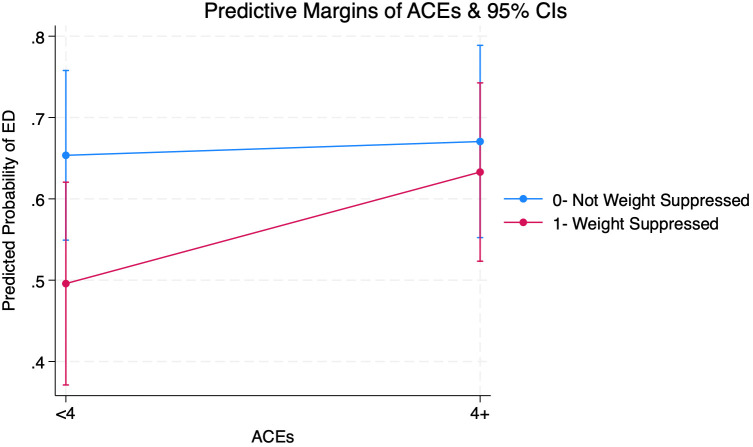
Adverse childhood experiences (ACEs), such as childhood maltreatment and household dysfunction, are positively linked to substance use disorders (SUD), weight loss efforts, and maladaptive eating behaviors, including ultra-processed food addiction (UPFA) and eating disorder (ED) symptoms. However, the differential association of ACEs with UPFA by lifetime SUD history and ACEs with EDs by weight suppression- the discrepancy between an individual's highest and current weight/BMI in adulthood- have not been examined. Using logistic regression and marginal effects analysis, this cross-sectional study aimed to assess (1) cumulative ACEs as a risk factor for screening positive for UPFA and EDs, (2) lifetime SUD history as a moderator of the ACE-UPFA relationship, and (3) weight suppression as a moderator of the ACE-ED relationship. Among 287 adults presenting to a private practice offering nutrition counseling for EDs and SUD recovery, the presence of 4 or more ACEs (compared to <4 ACEs) significantly increased the odds of UPFA-positive screens (OR=1.99; CI=1.19-3.35; p=0.01) but not ED-positive screens (OR=1.36; CI=0.80-2.30, p=0.25). Additionally, the interaction between ACEs and SUD was significant to the UPFA outcome (p<0.01). Those with a self-reported lifetime history of SUD exhibited an increased probability of UPFA-positive screens in the presence of 4 or more ACEs. Meanwhile, the probability of UPFA-positive screens remained unchanged among those who did not report a lifetime SUD history. Cumulative ACEs did not significantly predict ED-positive screens, and the ACE-weight suppression interaction did not meet the threshold for significance. Overall findings underscore the cross-vulnerability between addictive behaviors and the potential importance of integrating nutrition interventions in addiction treatment for those with ACEs.
Keywords: adverse childhood experiences; eating disorder; food addiction; moderation; substance use disorder; ultra-processed food; weight suppression.
Copyright © 2025 Wiss, Tran and LaFata.
Conflict of interest statement
Author DW was employed by the company Nutrition in Recovery LLC. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Structural equation modeling of adverse childhood experiences, ultra-processed food intake, and symptoms of post-traumatic stress disorder, ultra-processed food addiction, and eating disorder among adults seeking nutrition counseling in Los Angeles, CA.Appetite. 2025 Apr 1;208:107938. doi: 10.1016/j.appet.2025.107938. Epub 2025 Mar 2. Appetite. 2025. PMID: 40031408
-
Perceived social support moderates the association between household dysfunction adverse childhood experiences (ACEs) and self-reported drug use among men who have sex with men in Los Angeles, California.Int J Drug Policy. 2022 Dec;110:103899. doi: 10.1016/j.drugpo.2022.103899. Epub 2022 Nov 2. Int J Drug Policy. 2022. PMID: 36334318
-
Adverse childhood experiences among adults with eating disorders: comparison to a nationally representative sample and identification of trauma.J Eat Disord. 2022 May 20;10(1):72. doi: 10.1186/s40337-022-00594-x. J Eat Disord. 2022. PMID: 35596196 Free PMC article.
-
Adverse childhood experiences (ACEs) and substance use disorder (SUD): A scoping review.Drug Alcohol Depend. 2021 Apr 1;221:108563. doi: 10.1016/j.drugalcdep.2021.108563. Epub 2021 Jan 29. Drug Alcohol Depend. 2021. PMID: 33561668
-
Adverse childhood experiences and related outcomes among adults experiencing homelessness: a systematic review and meta-analysis.Lancet Public Health. 2021 Nov;6(11):e836-e847. doi: 10.1016/S2468-2667(21)00189-4. Epub 2021 Sep 30. Lancet Public Health. 2021. PMID: 34599894
Cited by
-
Effects of adverse childhood experiences on health behaviors among medical students: A cross-sectional study.Medicine (Baltimore). 2025 Jul 11;104(28):e43259. doi: 10.1097/MD.0000000000043259. Medicine (Baltimore). 2025. PMID: 40660598 Free PMC article.
References
-
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. . Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults the adverse childhood experiences (ACE) study. Am J Prev Med. (1998) 14:245–58. doi: 10.1016/s0749-3797(98)00017-8 - DOI - PubMed
-
- Skiendzielewski K, Forke CM, Sarwer DB, Noll JG, Wheeler DC, Henry KA, et al. . The intersection of adverse childhood experiences and neighborhood determinants of health: An exploratory spatial analysis. psychol Trauma: Theory Res Pract Policy. (2024) 16:S125–32. doi: 10.1037/tra0001320 - DOI - PMC - PubMed
-
- Merrick MT, Ford DC, Ports KA, Guinn AS, Chen J, Klevens J, et al. . Vital signs: estimated proportion of adult health problems attributable to adverse childhood experiences and implications for prevention — 25 states, 2015–2017. Morb Mortal Wkly Rep. (2019) 68:999–1005. doi: 10.15585/mmwr.mm6844e1 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous