

Maternal and neonatal outcomes of pregnancies after metabolic bariatric surgery: a retrospective population-based study
- PMID: 40213500
- PMCID: PMC11982497
- DOI: 10.1016/j.lanepe.2025.101263
Maternal and neonatal outcomes of pregnancies after metabolic bariatric surgery: a retrospective population-based study
Abstract
Background: The incidence of post metabolic bariatric surgery (BS) pregnancies is rising. Previous studies provided conflicting results regarding the risk of prematurity, stillbirth, perinatal death and the optimal time from BS to conception. This study examined maternal and neonatal outcomes of post-BS pregnancies and influencing factors.
Methods: Nationwide retrospective study of all post-BS pregnancies in France from January 1st 2013 to December 31st 2022. We compared 55,941 post-BS pregnancies with 223,712 controls matched on delivery date, parity, age, obesity, hypertension, diabetes, and socio-economic status (1:4 ratio) using generalized estimating equations. We also compared 11,777 post-BS pregnancies with 11,777 pre-BS pregnancies in the same women, using conditional logistic regression. Maternal outcomes included gestational hypertension, preeclampsia, and gestational diabetes. Neonatal outcomes included small-for-gestational-age (SGA), prematurity, stillbirth, and perinatal death. We tested for interactions with BS type, BS to pregnancy time interval and malnutrition.
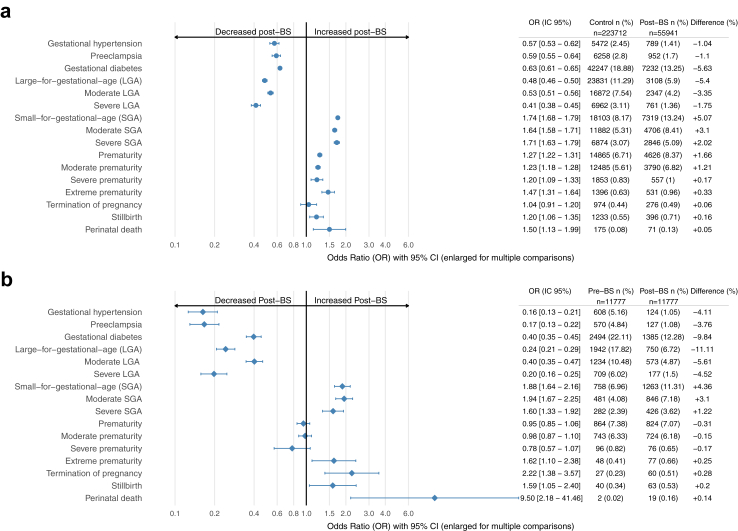
Findings: Post-BS pregnancies were associated with reduced risk of gestational hypertension (odds ratio [OR] 0.57 [95% CI 0.53-0.62]), preeclampsia (OR 0.59 [0.55-0.64]), and gestational diabetes (OR 0.64 [0.62-0.66]) as compared with control. Similar but stronger risk reductions were observed compared with pre-BS pregnancies. Risk of SGA was increased (OR 1.74 [1.68-1.79]) as compared with controls and pre-BS pregnancies (OR 1.88 [1.64-2.16]). Risk of prematurity was increased (OR 1.27 [1.22-1.31]) as compared with controls but not pre-BS pregnancies (OR 0.95 [0.85-1.06]). Compared with controls, risk of stillbirth was increased (OR 1.2 [1.06-1.35]), mediated by SGA, as was perinatal death (OR 1.5 [1.13-1.99]), mediated by both prematurity and SGA. Increased SGA risk compared to controls was higher with malnutrition (OR: 2.38 [1.96, 2.88], pinteraction <0.0001), with <6 months (OR: 1.95 [1.72, 2.21], pinteraction = 0.01) or 6-12 months between BS and pregnancy (OR: 1.86 [1.70, 2.04], pinteraction = 0.02) and with gastric bypass (OR: 1.88 [1.77-2.00], pinteraction = 0.027). Increased prematurity risk compared to controls was higher with malnutrition (2.45 [1.99, 3.00], pinteraction <0.0001) and gastric bypass (OR: 1.46 [1.36-1.57], pinteraction = 0.0003).
Interpretation: Post-BS compared with pre-BS or control pregnancies were associated with reduced risk of maternal adverse outcomes but increased risk of neonatal adverse events. The risks of SGA and prematurity are higher with shorter intervals between BS and conception, gastric bypass, and malnutrition. Post-BS pregnancies could be considered high risk, requiring close nutritional and obstetrical monitoring.
Funding: Support from INSERM and the French Ministry of Health (Messidore 2022 n°97).
Keywords: Bariatric surgery; Gastric bypass; Gestational diabetes; Gestational hypertension; Malnutrition; Neonatal death; Nutrition; Obesity; Preeclampsia; Pregnancy; Prematurity; Sleeve gastrectomy; Small-for-gestational age.
© 2025 The Authors.
Conflict of interest statement
PBL, BL, CC, BS, LRS, ELU, SK, GG, AAX, AT, BH and CRL received support from INSERM and the French Ministry of Health (Messidore 2022 no. 97 - Innovative methodologies, devices, tools and research in clinical trials using health data and biobanks) as reported in the funding section. SC holds shares in ALIFERT, JELLYNOV companies and received personal fees from Bariatek, Novonordisk, Eli Lilly, Pfizer, Fresenius Kabi, Ipsen Pharma, Janssen-Cilag, Boehringer Ingelheim and Novartis. AL received payments from Johnson & Johnson, Medtronic and Gore for the organization of surgical workshop for bariatric surgeons and support from Novo Nordisk for attending congress. LR, TP, JN have nothing to declare.
Figures



References
-
- Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
LinkOut - more resources
Full Text Sources
