

Assessment of a Polygenic Risk Score in Screening for Prostate Cancer
- PMID: 40214032
- PMCID: PMC7617604
- DOI: 10.1056/NEJMoa2407934
Assessment of a Polygenic Risk Score in Screening for Prostate Cancer
Abstract
Background: The incidence of prostate cancer is increasing. Screening with an assay of prostate-specific antigen (PSA) has a high rate for false positive results. Genomewide association studies have identified common germline variants in persons with prostate cancer, which can be used to calculate a polygenic risk score associated with risk of prostate cancer.
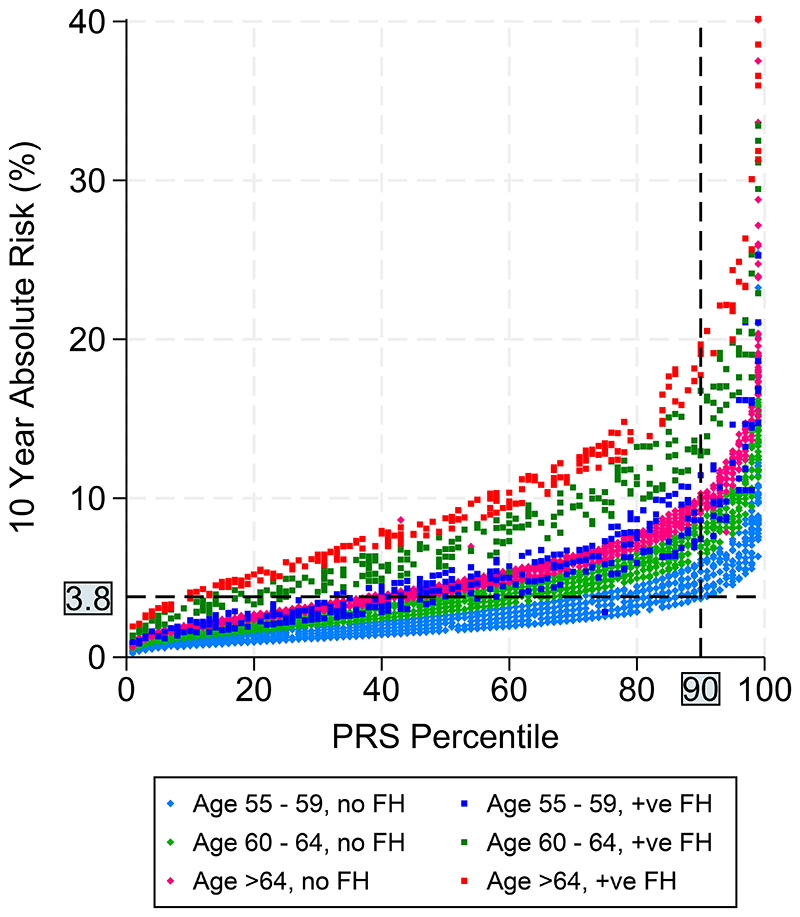
Methods: We recruited persons 55 to 69 years of age from primary care centers in the United Kingdom. Using germline DNA extracted from saliva, we derived polygenic risk scores from 130 variants known to be associated with an increased risk of prostate cancer. Participants with a polygenic risk score in the 90th percentile or higher were invited to undergo prostate cancer screening with multiparametric magnetic resonance imaging (MRI) and transperineal biopsy, irrespective of PSA level.
Results: Among 40,292 persons invited to participate, 8953 (22.2%) expressed interest in participating and 6393 had their polygenic risk score calculated; 745 (11.7%) had a polygenic risk score in the 90th percentile or higher and were invited to undergo screening. Of these 745 participants, 468 (62.8%) underwent MRI and prostate biopsy; prostate cancer was detected in 187 participants (40.0%). The median age at diagnosis was 64 years (range, 57 to 73). Of the 187 participants with cancer, 103 (55.1%) had prostate cancer classified as intermediate or higher risk according to the 2024 National Comprehensive Cancer Network (NCCN) criteria, so treatment was indicated; cancer would not have been detected in 74 (71.8%) of these participants according to the prostate cancer diagnostic pathway currently used in the United Kingdom (high PSA level and positive MRI results). In addition, 40 of the participants with cancer (21.4%) had disease classified as unfavorable intermediate risk or as high or very high risk according to NCCN criteria.
Conclusions: In a prostate cancer screening program involving participants in the top decile of risk as determined by a polygenic risk score, the percentage found to have clinically significant disease was higher than the percentage that would have been identified with the use of PSA or MRI. (Funded by the European Research Council Seventh Framework Program and others; BARCODE1 ClinicalTrials.gov number, NCT03857477.).
Copyright © 2025 Massachusetts Medical Society.
Figures


Comment in
-
Screening for Prostate Cancer with a Polygenic Risk Score.N Engl J Med. 2025 Aug 21;393(8):831. doi: 10.1056/NEJMc2507786. N Engl J Med. 2025. PMID: 40834316 No abstract available.
-
Screening for Prostate Cancer with a Polygenic Risk Score.N Engl J Med. 2025 Aug 21;393(8):831. doi: 10.1056/NEJMc2507786. N Engl J Med. 2025. PMID: 40834317 No abstract available.
-
Screening for Prostate Cancer with a Polygenic Risk Score.N Engl J Med. 2025 Aug 21;393(8):831-832. doi: 10.1056/NEJMc2507786. N Engl J Med. 2025. PMID: 40834318 No abstract available.
-
Screening for Prostate Cancer with a Polygenic Risk Score. Reply.N Engl J Med. 2025 Aug 21;393(8):832. doi: 10.1056/NEJMc2507786. N Engl J Med. 2025. PMID: 40834319 No abstract available.
-
Polygenic risk score (PRS) as prostate cancer screening: ready for primetime?Ann Transl Med. 2025 Aug 31;13(4):39. doi: 10.21037/atm-25-84. Epub 2025 Aug 26. Ann Transl Med. 2025. PMID: 40949682 Free PMC article. No abstract available.
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
-
- Andriole GL, Crawford ED, Grubb RL, 3rd, et al. Prostate cancer screening in the randomized Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial: mortality results after 13 years of follow-up. Journal of the National Cancer Institute. 2012;104(2):125–32. doi: 10.1093/jnci/djr500. - DOI - PMC - PubMed
-
- Cancer Research UK. 2024. https://www.cancerresearchuk.org/health-professional/cancer-statistics/s... .
-
- Asif A, Nathan A, Ng A, et al. Comparing biparametric to multiparametric MRI in the diagnosis of clinically significant prostate cancer in biopsy-naive men (PRIME): a prospective, international, multicentre, non-inferiority within-patient, diagnostic yield trial protocol. BMJ Open. 2023;13(4):e070280. doi: 10.1136/bmjopen-2022-070280. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous