

Effective coverage for maternal health: operationalising effective coverage cascades for antenatal care and nutrition interventions for pregnant women in seven low- and middle-income countries
- PMID: 40214129
- PMCID: PMC11987578
- DOI: 10.7189/jogh.15.04041
Effective coverage for maternal health: operationalising effective coverage cascades for antenatal care and nutrition interventions for pregnant women in seven low- and middle-income countries
Abstract
Background: Efforts to improve maternal health have focused on measuring health and nutrition service coverage. Despite improvements in service coverage, maternal mortality rates remain high. This suggests that coverage indicators alone do not fully capture the quality of care and may overestimate the health benefits of a service. Effective coverage (EC) cascades have been proposed as an approach to capture service quality within population-based coverage measures, but the proposed maternal health EC cascades have not been operationalised. This study aims to operationalise the effective coverage cascades for antenatal care (ANC) and maternal nutrition services using existing data from low- and middle-income countries (LMICs).
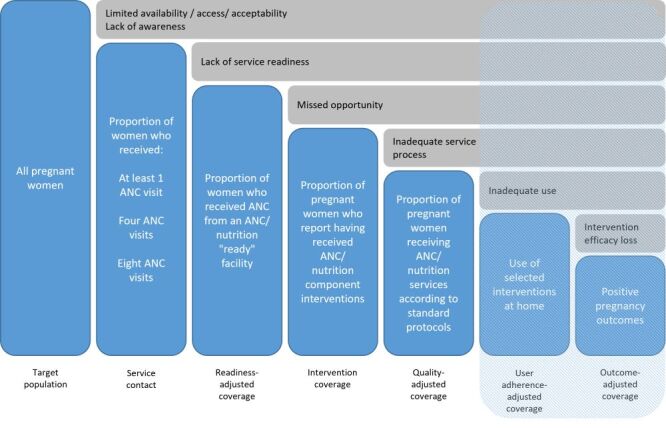
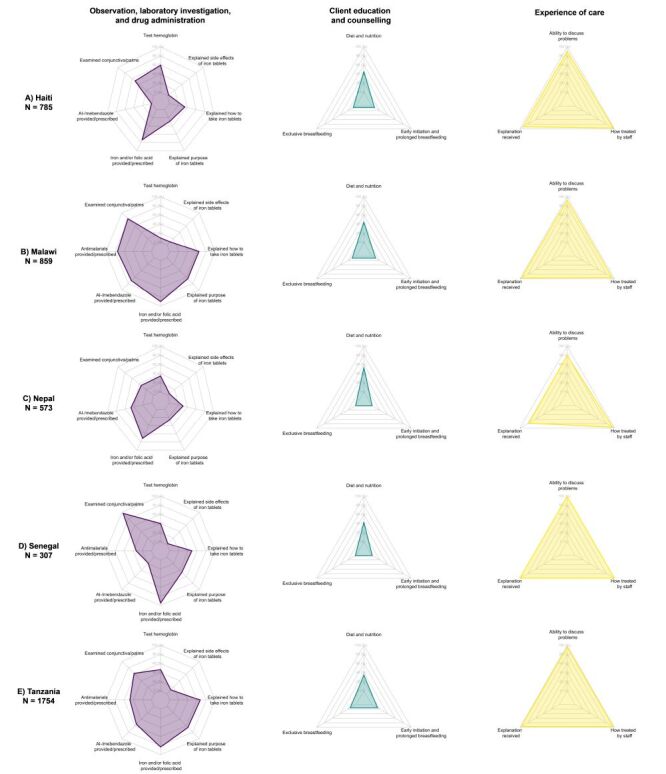
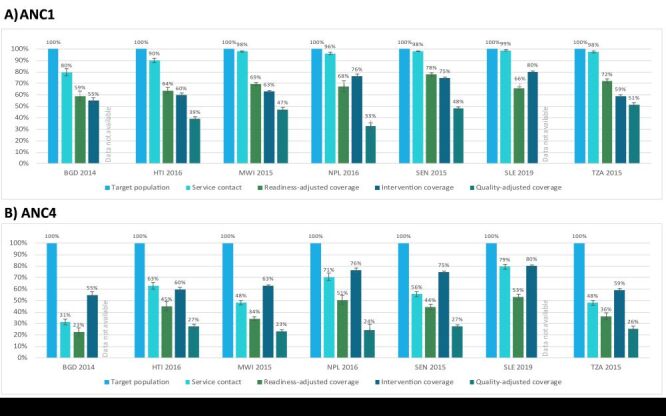
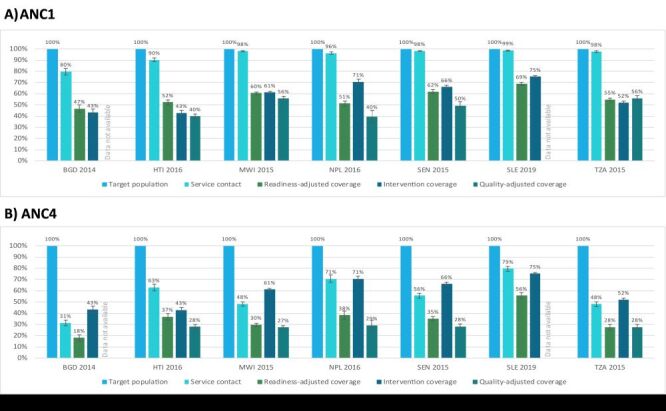
Methods: We used household surveys and health facility assessments from seven LMICs to estimate EC cascades for ANC and maternal nutrition services provided during ANC visits. We developed theoretical coverage cascades, defined health facility readiness and provision/experience of care scores and linked the facility-based scores to household survey data based on geographic domain and facility type. We then estimated the coverage cascade steps for each service by country.
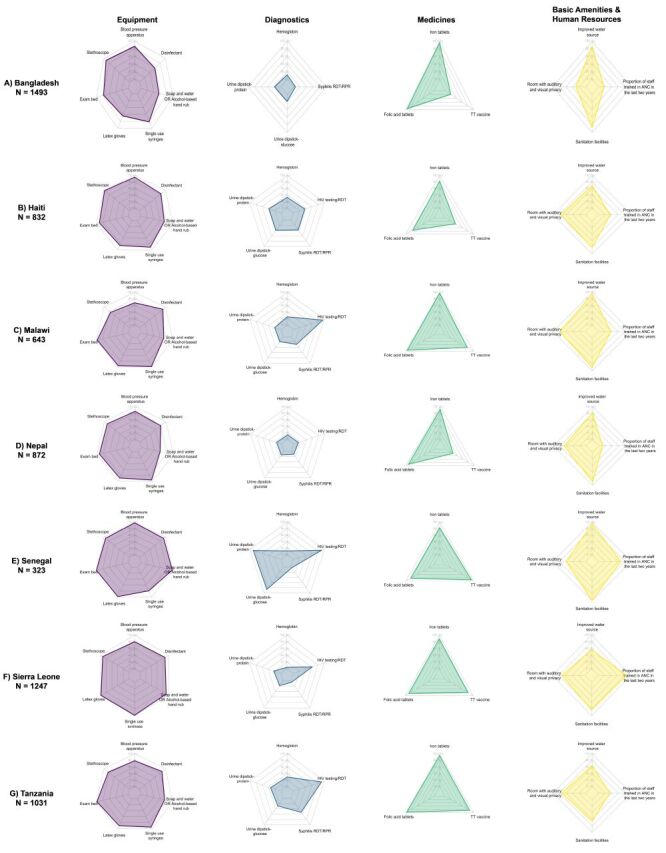
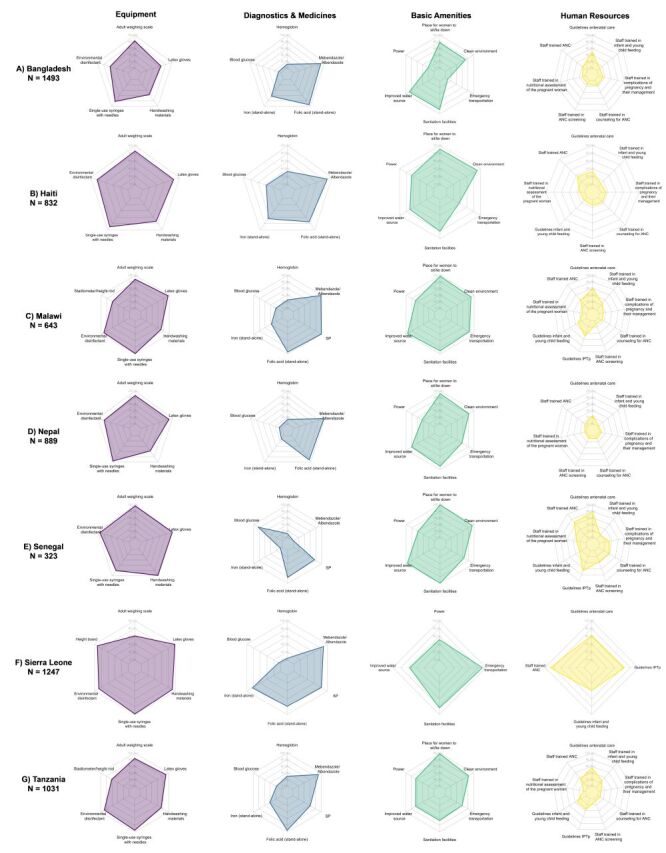
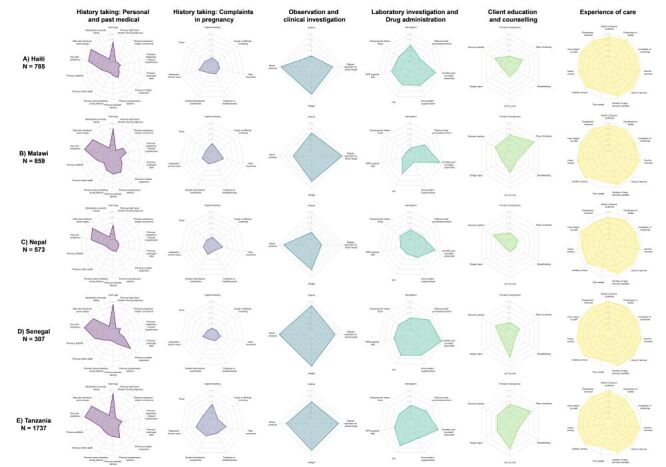
Results: Service contact coverage for at least one ANC visit (ANC1) was high, ranging from 80% in Bangladesh to 99% in Sierra Leone. However, there was a substantial drop in coverage from service contact to readiness-adjusted coverage, and a further drop to quality-adjusted coverage for all countries. For ANC1, from service contact to quality-adjusted coverage, there was an average net decline of 52 percentage points. For ANC1 maternal nutrition services, there was an average net decline of 48 percentage points from service contact to quality-adjusted coverage. This pattern persisted across cascades. Further exploration revealed that gaps in service readiness including lack of provider training, and gaps in provision/experience of care such as limited nutrition counselling were core contributors to the drops in coverage observed.
Conclusions: The cascade approach provided useful summary measures that identified major barriers to EC. However, detailed measures underlying the steps of the cascade are likely needed to support evidence-based decision-making with more actionable information. This analysis highlights the importance of understanding bottlenecks in achieving health outcomes and the inter-connectedness of service access and service quality to improve health in LMICs.
Copyright © 2025 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and all authors except Rebecca Heidkamp disclose no relevant interests. Rebecca Heidkamp reports the following activities: a leadership role with the Society for Implementation Science for Nutrition and membership in the WHO-UNICEF Technical Experts Group on Nutrition Measurement.
Figures

Similar articles
-
Building an effective coverage cascade for antenatal care: linking of household survey and health facility assessment data in eight low- and middle-income countries.J Glob Health. 2025 Feb 14;15:04048. doi: 10.7189/jogh.15.04048. J Glob Health. 2025. PMID: 39950560 Free PMC article.
-
High coverage but low quality of maternal and newborn health services in the coverage cascade: who is benefitted and left behind in accessing better quality health services in Nepal?Reprod Health. 2022 Jul 19;19(1):163. doi: 10.1186/s12978-022-01465-z. Reprod Health. 2022. PMID: 35854265 Free PMC article.
-
Quality of antenatal care service provision in health facilities across sub-Saharan Africa: Evidence from nationally representative health facility assessments.J Glob Health. 2017 Dec;7(2):021101. doi: 10.7189/jogh.07.021101. J Glob Health. 2017. PMID: 29163936 Free PMC article.
-
Trends of antenatal care during pregnancy in low- and middle-income countries: Findings from the global network maternal and newborn health registry.Semin Perinatol. 2019 Aug;43(5):297-307. doi: 10.1053/j.semperi.2019.03.020. Epub 2019 Mar 16. Semin Perinatol. 2019. PMID: 31005357 Free PMC article. Review.
-
Interventions to enhance healthcare utilisation among pregnant women to reduce maternal mortality in low- and middle-income countries: a review of systematic reviews.BMC Public Health. 2023 Sep 6;23(1):1734. doi: 10.1186/s12889-023-16558-y. BMC Public Health. 2023. PMID: 37674154 Free PMC article. Review.
References
-
- United Nations. SDG 3: Ensure healthy lives and promote wellbeing for all at all ages. Available: https://sdgs.un.org/goals/goal3. Accessed: 28 June 2022.
-
- World Health Organization, UNICEF, UNFPA, World Bank Group, United Nations Population Division. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Geneva, Switzerland: World Health Organization; 2023.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
