

Trends in Abortion Rates in Ontario, Canada
- PMID: 40214991
- PMCID: PMC11992605
- DOI: 10.1001/jamanetworkopen.2025.4516
Trends in Abortion Rates in Ontario, Canada
Abstract
Importance: Following decades-long declines, significant increases in abortion rates have been reported in some jurisdictions from 2020 to 2023, but it is not yet known whether these trends are occurring in Canada.
Objective: To assess abortion rates in Ontario from 2012 to 2022 and to examine trend changes associated with mifepristone availability, the COVID-19 pandemic, and postpandemic periods.
Design, setting, and participants: This population-based interrupted time series cohort study examined all medication and procedural abortions provided in Ontario from January 1, 2012, to December 31, 2022, to females aged 15 to 44 years with provincial insurance coverage, identified using linked health administrative data that included records from practitioner billings, inpatient and outpatient hospital services, same-day surgeries, and outpatient prescription dispensations.
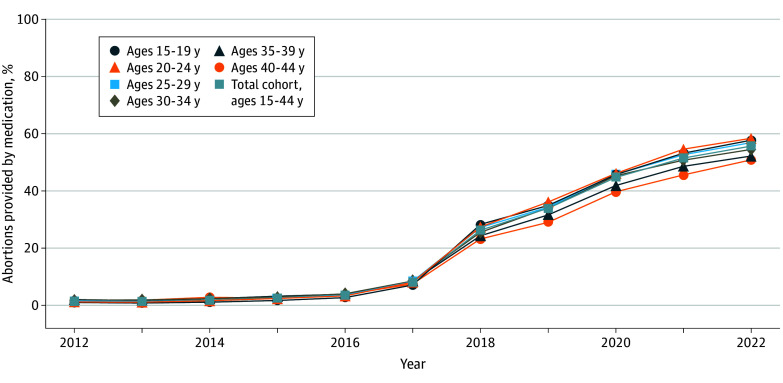
Exposure: Availability of mifepristone regulated as a normal (ie, prescribed by an authorized prescriber without additional certification or registration and dispensed by a pharmacist) prescription medication (in November 2017) and the COVID-19 pandemic period (from March 2020 to December 2021).
Main outcomes and measures: The main outcome was the abortion rate (number of abortions per 1000 females per year) overall and within age strata, using an interrupted time series design.
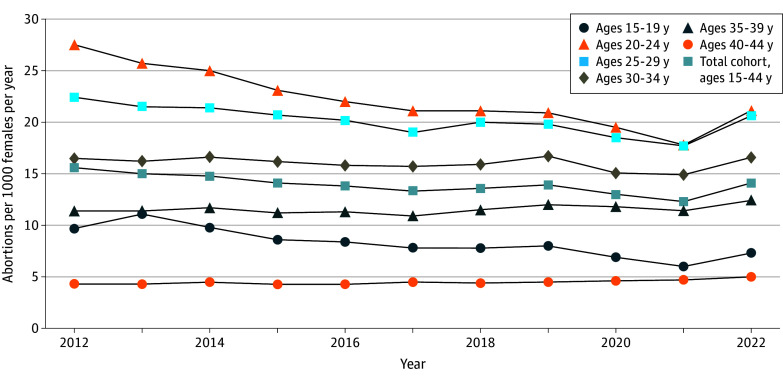
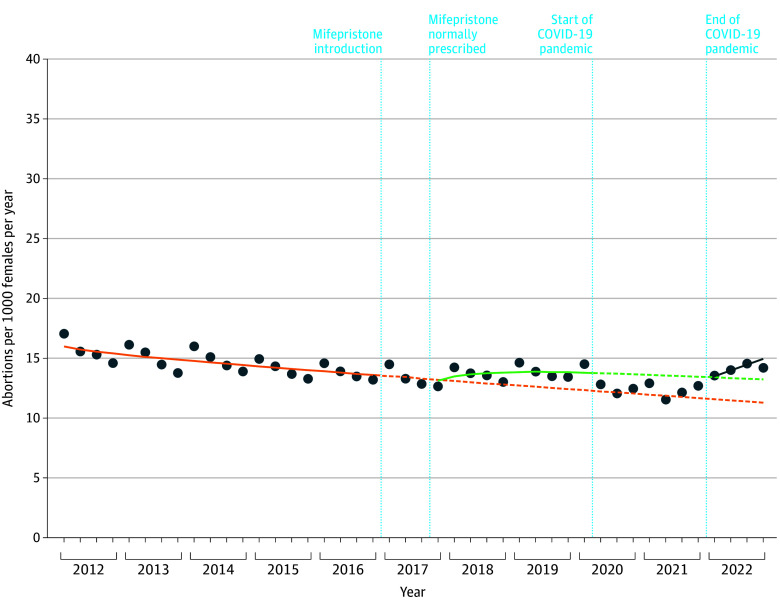
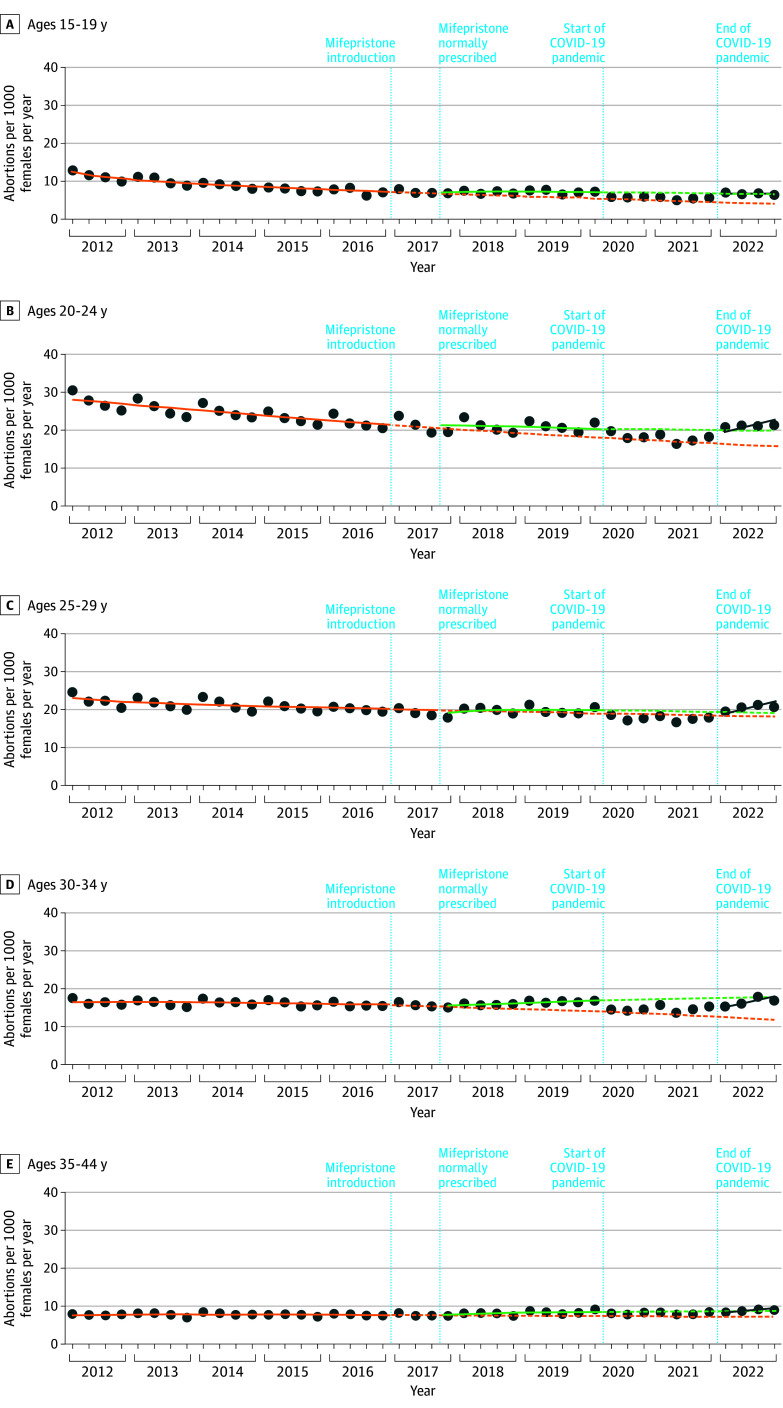
Results: Of 422 867 medication and procedural abortions identified using data from health records of 225 540 reproductive-aged females (mean [SD] age, 28.5 [6.6] years), the abortion rate declined steadily from 15.6 abortions per year per 1000 females, aged 15 to 44 years, in 2012 to 12.3 in 2021 and then increased to 14.1 in 2022. When mifepristone was introduced in 2017 as a normal prescription medication, no immediate change in the abortion rate (-0.1 [95% CI, -0.7 to 0.8]) and a nonsignificant slope increase (0.6 [95% CI, -0.5 to 0.7]) were found. However, this trend resulted in an additional 1.5 (95% CI, 0.3-2.6) abortions per 1000 females by the first quarter of 2020 compared with premifepristone trends; rates increased more among those aged 15 to 19 years, less among those aged 35 to 44 years, and did not increase for those aged 25 to 29 years. During the pandemic period, abortion rates decreased by 1.2 (95% CI, -2.5 to -0.8), most pronounced among those aged 20 to 34 years. Compared with expected rates based on premifepristone trends, 5-year availability of normally prescribed mifepristone was associated with a rate difference of 1.9 (95% CI, 0.7-5.4) in 2022, with a greater increase among those aged 20 to 24 years (4.2 [95% CI, 1.5-9.0]) and no change among those aged 25 to 29 years (1.0 [95% CI, -1.7 to 6.2]). The increased abortion rate in 2022 was consistent with 5-year trends following normally prescribed mifepristone, although social forces potentially impacting international rates may have contributed.
Conclusions and relevance: This study found that, following longstanding declines, abortion rates in Ontario gradually increased with mifepristone availability in 2017 in Ontario. Following a pandemic-related decrease in rates (in 2020 and 2021), substantial increases in abortion rates reported elsewhere from 2020 to 2023 did not occur in Ontario as of 2022, suggesting that Ontario's health services environment and Canada's regulatory and policy approach to preserving reproductive health services may have helped stabilize abortion rates. Future research is needed to understand how sociocultural changes affecting abortion service use elsewhere may be affecting contraception access and use and thus abortion rates in Canada.
Conflict of interest statement
Figures
Similar articles
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Risk of thromboembolism in patients with COVID-19 who are using hormonal contraception.Cochrane Database Syst Rev. 2023 Jan 9;1(1):CD014908. doi: 10.1002/14651858.CD014908.pub2. Cochrane Database Syst Rev. 2023. Update in: Cochrane Database Syst Rev. 2023 May 15;5:CD014908. doi: 10.1002/14651858.CD014908.pub3. PMID: 36622724 Free PMC article. Updated.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Acceptability of misoprostol-only medication abortion dispensed by mail-order or retail pharmacy: a qualitative study based on in-depth interviews in the United States.Sex Reprod Health Matters. 2025 Dec;33(1):2522567. doi: 10.1080/26410397.2025.2522567. Epub 2025 Jul 25. Sex Reprod Health Matters. 2025. PMID: 40539380 Free PMC article.
Cited by
-
Changes in local access to mifepristone dispensed by community pharmacies for medication abortion in Ontario: a population-based repeated cross-sectional study.CMAJ. 2025 Apr 6;197(13):E345-E354. doi: 10.1503/cmaj.241505. CMAJ. 2025. PMID: 40194816 Free PMC article.
References
-
- Termination of pregnancy statistics: year ending December 2023. Public Health Scotland . May 28, 2024. Accessed October 2, 2024. https://publichealthscotland.scot/publications/termination-of-pregnancy-...
-
- Accredited official statistics. Abortion statistics, England and Wales: 2022. Office for Health Improvement & Disparities, UK Department of Health and Social Care . GOV.UK. December 18, 2024. Accessed March 8, 2025. https://www.gov.uk/government/statistics/abortion-statistics-for-england...
-
- Interruptions of pregnancy. Federal Statistical Office, Swiss Confederation . Accessed October 4, 2024. https://www.bfs.admin.ch/bfs/fr/home/statistiques/sante/etat-sante/repro...
-
- Maddow-Zimet I, Gibson C; Guttmacher Institute . Policy analysis. Despite bans, number of abortions in the United States increased in 2023. March 2024. Accessed October 2, 2024. https://www.guttmacher.org/2024/03/despite-bans-number-abortions-united-...
-
- Espey E, Teal S, Peipert JF. A statement on abortion by 900 professors of obstetrics and gynecology after the reversal of Roe vWade. Am J Obstet Gynecol. 2024;230(1):10-11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
