

The association of albumin-corrected anion gap and acute kidney injury in heart failure patients: a competing risk model analysis
- PMID: 40217175
- PMCID: PMC11987305
- DOI: 10.1186/s12872-025-04723-7
The association of albumin-corrected anion gap and acute kidney injury in heart failure patients: a competing risk model analysis
Abstract
Background: The combination of heart failure (HF) and acute kidney injury (AKI) increases the mortality of patients. It is critical to identify HF patients who may have a high risk for AKI. Albumin-corrected anion gap (ACAG) is a new indicator, but there are no studies on ACAG and the risk of AKI in HF patients.
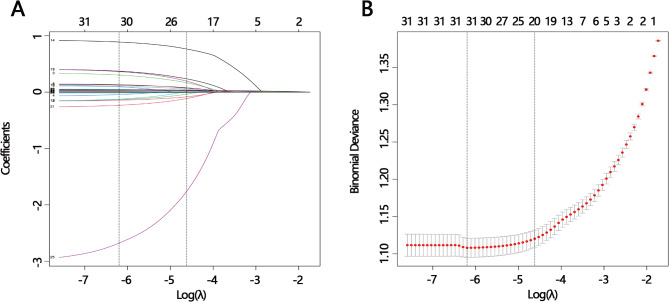
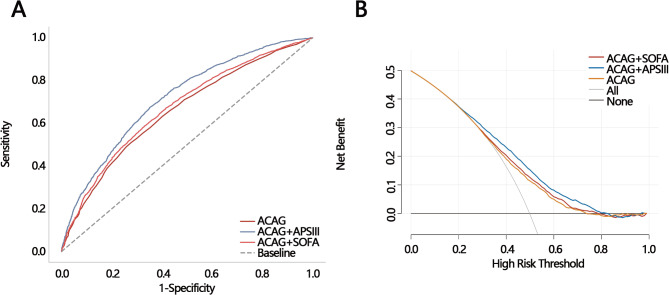
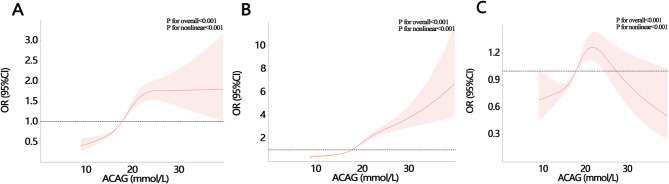
Methods: Data for HF patients was obtained from the MIMIC-IV database. Receiver operating characteristic (ROC) analysis and decision curve analysis (DCA) were employed to evaluate the clinical value of ACAG in predicting AKI risk. Logistic regression analysis and restricted cubic spline (RCS) curve were conducted to explore the relationship between ACAG and AKI. A competing risk model was developed to further investigate the relationship between ACAG on AKI.
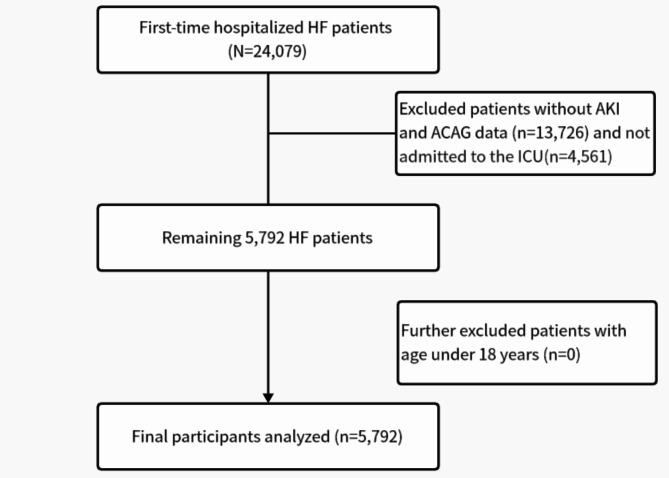
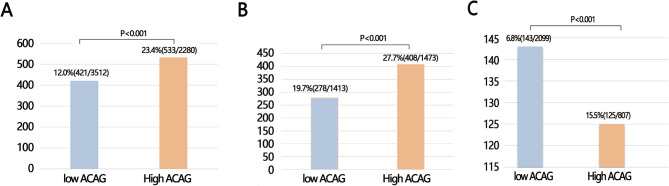
Results: The study analyzed 5,972 HF patients, with 49.82% (2886/5972) suffering from AKI. The prediction performance of ACAG on AKI was good (AUC:0.656). Continuous ACAG was associated with AKI after adjusting for various significant variables (Model 1: OR = 1.094, 95%CI: 1.078-1.110; Model 2: OR = 1.150, 95%CI: 1.133-1.166; Model 3: OR = 1.035, 95%CI. 1.017-1.054). All High ACAG groups showed a higher risk of AKI (all P < 0.001). ACAG was also linked to in-hospital mortality (P < 0.001). The competing risks model revealed that high ACAG was still a risk factor for AKI when in-hospital mortality served as a competing risk event (P < 0.001).
Conclusion: High ACAG was associated with the risk of AKI in HF patients. Clinicians can risk-stratify HF patients by combining ACAG levels.
Keywords: Acute kidney injury; Albumin-corrected anion gap; Competing risk; Heart failure; Prognosis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Ethics Committee of Hangzhou Lin’an District Hospital of Traditional Chinese Medicine deemed that this research is based on open-source data, so the need for ethics approval was waived. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Clinical trial: Not applicable.
Figures

Similar articles
-
Association of albumin-corrected anion gap with mortality in ICU patients with heart failure and acute kidney injury: analysis of the MIMIC-IV database.Eur J Med Res. 2025 Aug 13;30(1):745. doi: 10.1186/s40001-025-03035-y. Eur J Med Res. 2025. PMID: 40796876 Free PMC article.
-
Independent prognostic importance of the albumin-corrected anion gap in critically ill patients with congestive heart failure: a retrospective study from MIMIC-IV database.BMC Cardiovasc Disord. 2024 Dec 20;24(1):735. doi: 10.1186/s12872-024-04422-9. BMC Cardiovasc Disord. 2024. PMID: 39707198 Free PMC article.
-
The association between Albumin-Corrected Anion Gap (ACAG) and the risk of acute kidney injury in patients with acute pancreatitis: A retrospective analysis based on the MIMIC-IV database.PLoS One. 2025 Aug 22;20(8):e0330458. doi: 10.1371/journal.pone.0330458. eCollection 2025. PLoS One. 2025. PMID: 40844993 Free PMC article.
-
Prognostic value of anion gap for patients with heart failure: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2024 Dec 20;24(1):727. doi: 10.1186/s12872-024-04420-x. BMC Cardiovasc Disord. 2024. PMID: 39707227 Free PMC article.
-
Risk for Incident Heart Failure: A Subject-Level Meta-Analysis From the Heart "OMics" in AGEing (HOMAGE) Study.J Am Heart Assoc. 2017 May 2;6(5):e005231. doi: 10.1161/JAHA.116.005231. J Am Heart Assoc. 2017. PMID: 28465299 Free PMC article. Review.
Cited by
-
Association of albumin-corrected anion gap with mortality in ICU patients with heart failure and acute kidney injury: analysis of the MIMIC-IV database.Eur J Med Res. 2025 Aug 13;30(1):745. doi: 10.1186/s40001-025-03035-y. Eur J Med Res. 2025. PMID: 40796876 Free PMC article.
References
-
- Ronco C, Bellomo R, Kellum JA. Acute kidney injury. Lancet. 2019;394(10212):1949–64. - PubMed
-
- Cheungpasitporn W, Thongprayoon C, Kashani KB. Artificial intelligence in heart failure and acute kidney injury: emerging concepts and controversial dimensions. Cardiorenal Med. 2024;14(1):147–59. - PubMed
-
- Cook C, Cole G, Asaria P, Jabbour R, Francis DP. The annual global economic burden of heart failure. Int J Cardiol. 2014;171(3):368–76. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
