

Combined Pharmacological and surgical treatments for recurrent chemical peritonitis due to rupture of a bilateral mature cystic teratoma: a case report
- PMID: 40217218
- PMCID: PMC11987357
- DOI: 10.1186/s12905-025-03719-x
Combined Pharmacological and surgical treatments for recurrent chemical peritonitis due to rupture of a bilateral mature cystic teratoma: a case report
Abstract
Background: Mature cystic teratomas, a common type of benign ovarian tumors, are associated with complications such as twisting and tumor rupture; Rupture can cause severe chemical peritonitis, and no management policy has been established for the intraoperative and postoperative periods. Although peritoneal lavage and reoperation have been reported, the optimal treatment approach remains undetermined.
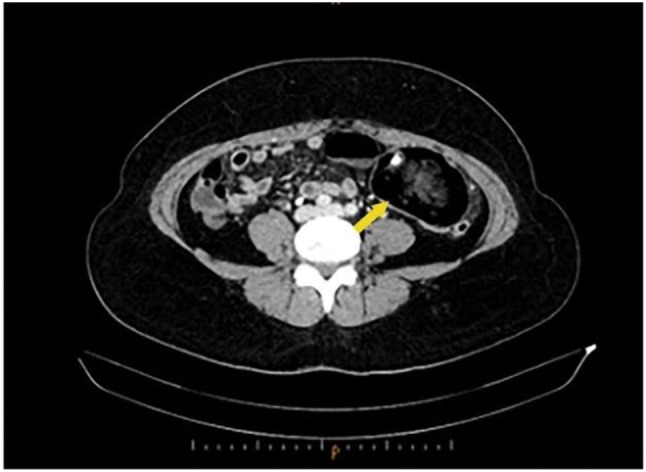
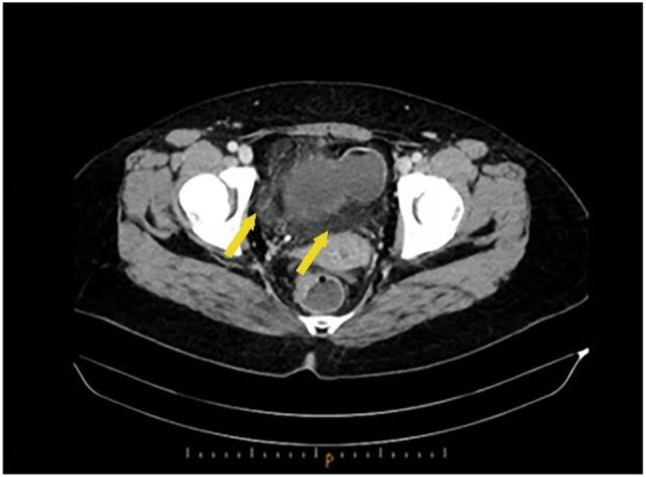
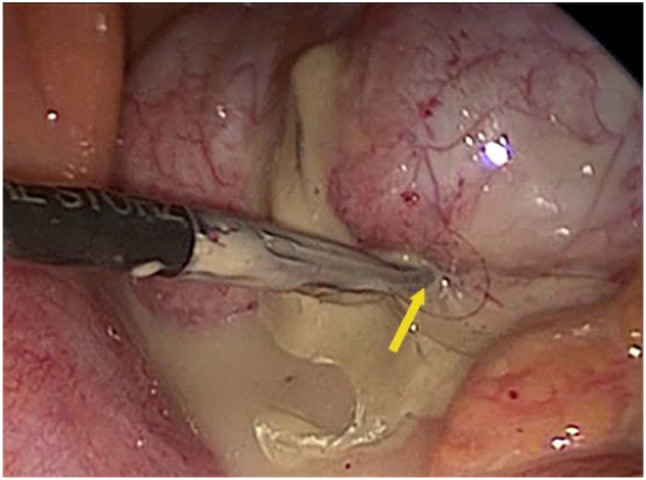
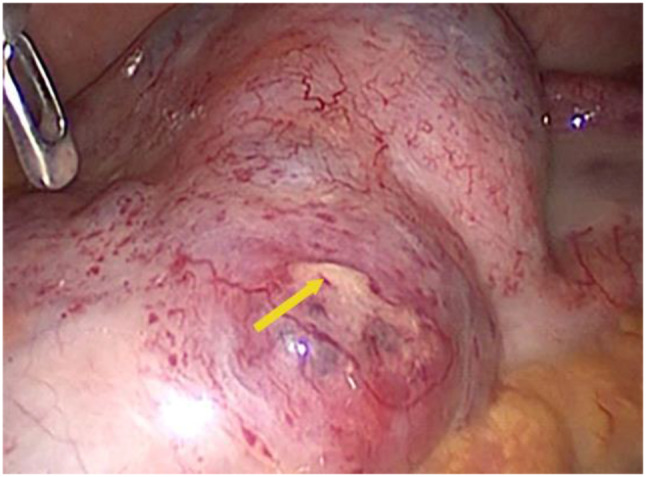
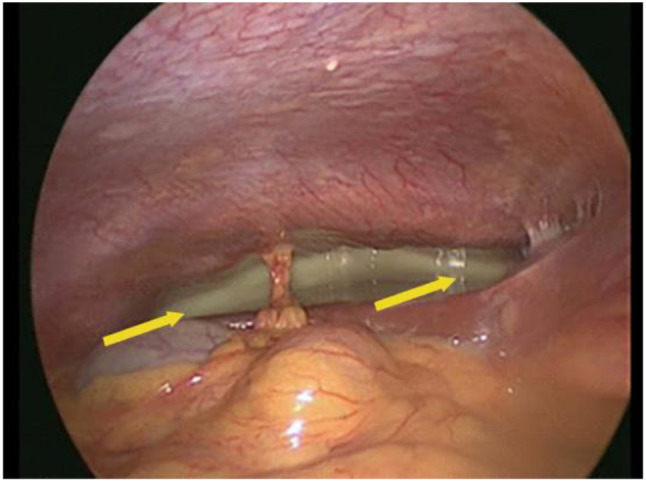
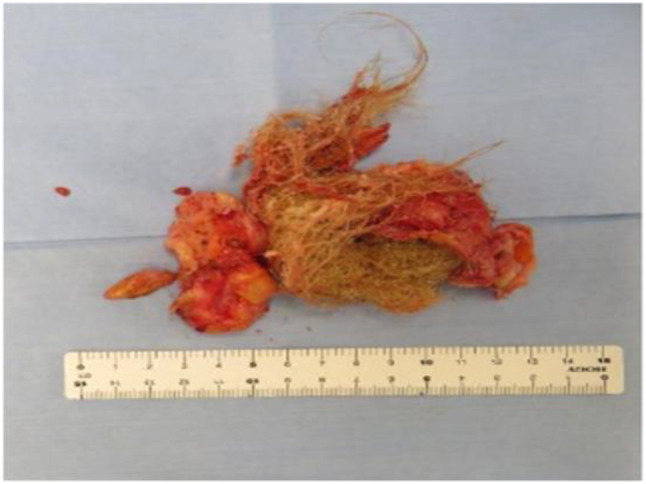
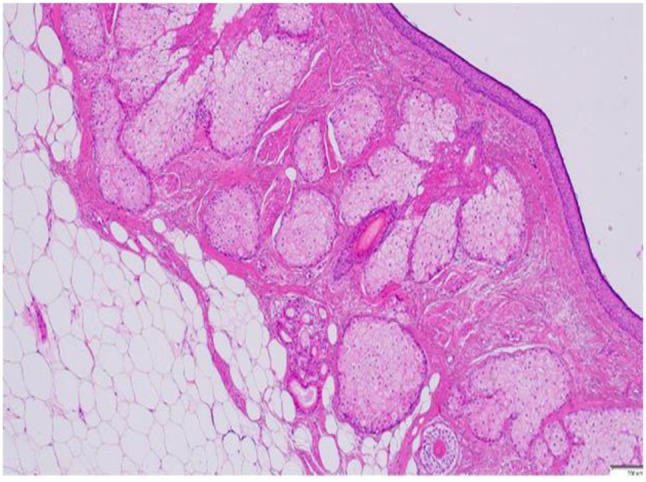
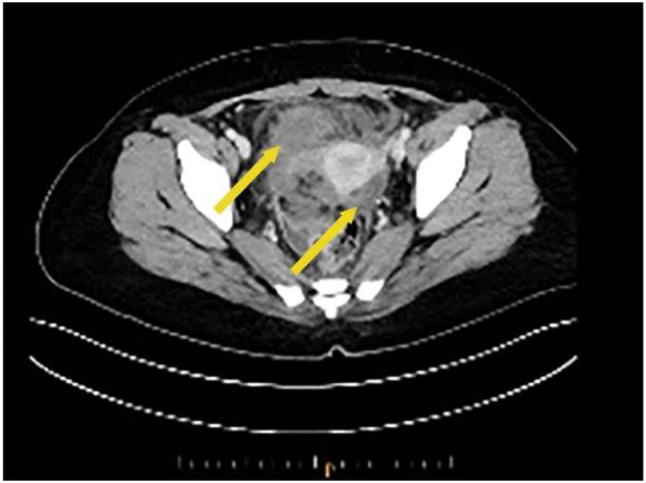
Case presentation: A 30-year-old woman (gravida 0, para 0, and no sexual history) presented with abdominal pain and fever. Blood examination revealed high levels of WBC 9200/µL and CRP 23.7 mg/dL, although hemoglobin was normal. Serum tumor marker levels were also elevated (CA125 58.5 U/mL, CA19-9 36117 U/mL). Abdominal computed tomography revealed bilateral ovarian tumors (92 and 68 mm in the right and left ovaries, respectively). Each tumor cavity had calcification with increased fatty tissue density. We performed laparoscopic surgery for suspected diagnosis of torsion or rupture of a mature cystic teratoma. Intraoperative findings showed spontaneous rupture followed by chemical peritonitis. Therefore, we performed removal of the bilateral adnexal tumors and peritoneal lavage with 3000 mL warm saline to remove fatty components from the abdominal cavity. We also inserted an intra-abdominal drain to remove the residual fatty components. Amoxicillin was also administered for 10 days after surgery. The inflammatory response decreased, and the fever diminished 1 day postoperatively. The patient was discharged on the 10th postoperative day. However, on the 20th postoperative day, the fever and abdominal pain recurred. WBC 16,700/µL, CRP 26.46 mg/dL and tumor marker (CA125 172.3 U/mL, CA19-9 225.2 U/mL) levels were high. Intravenous administration of Prophylactic antibiotics was initiated. As no bacteria were detected in the blood cultures, we started oral prednisolone (5 mg/day) to treat the recurrent chemical peritonitis-induced inflammation. The blood test results and symptoms gradually improved. The patient was discharged on the 37th postoperative day.
Conclusion: To date, no systematic review has focused on determining the treatment strategy for bilateral rupture of mature cystic teratomas and severe refractory chemical peritonitis. Treating the patient with laparoscopic surgery at the first occurrence and oral steroids for peritonitis recurrence can help avoid highly invasive treatments, such as reoperation or laparotomy.
Keywords: Chemical peritonitis; Fertility preservation; Laparoscopic surgery; Mature cystic teratoma; Spontaneous rupture.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This report was approved by the Hospital Ethics Committee of the University of Fukui Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Chemical peritonitis resulting from spontaneous rupture of a mature ovarian cystic teratoma: a case report.Acta Med Litu. 2019;26(4):217-226. doi: 10.6001/actamedica.v26i4.4207. Acta Med Litu. 2019. PMID: 32355460 Free PMC article.
-
Chemical peritonitis caused by an iatrogenic rupture of mature cystic teratoma of the ovary during labor: a report of a case didactic to all the maternity health care workers.J Matern Fetal Neonatal Med. 2011 Feb;24(2):388-90. doi: 10.3109/14767058.2010.482626. Epub 2010 May 12. J Matern Fetal Neonatal Med. 2011. PMID: 20459340
-
Severe chemical peritonitis caused by spontaneous rupture of an ovarian mature cystic teratoma: a case report.J Reprod Med. 2007 Oct;52(10):965-7. J Reprod Med. 2007. PMID: 17977177
-
Clinical characteristics and laparoscopic surgical outcomes of ovarian dermoid cysts complicated by spontaneous rupture: nine cases and a literature review.J Int Med Res. 2023 May;51(5):3000605231171023. doi: 10.1177/03000605231171023. J Int Med Res. 2023. PMID: 37138472 Free PMC article. Review.
-
Chemical peritonitis in pregnancy: An unusual presentation and review of the literature.J Obstet Gynaecol. 2016 May;36(4):496-7. doi: 10.3109/01443615.2015.1094039. Epub 2016 Jan 20. J Obstet Gynaecol. 2016. PMID: 26789232 Review. No abstract available.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
