

Cooking with the curriculum: a pilot culinary medicine program at the Larner College of Medicine
- PMID: 40217237
- PMCID: PMC11987183
- DOI: 10.1186/s12909-025-07103-z
Cooking with the curriculum: a pilot culinary medicine program at the Larner College of Medicine
Abstract
Background: Physicians are highly trusted sources of health advice, yet many feel unprepared to address nutrition with their patients due to a perceived lack of knowledge or confidence. In recent years, there has been increased recognition in medical education of lifestyle factors' impact on health outcomes in chronic diseases and the value of integrating diet-related interventions into patient care. This integration requires physicians and healthcare professionals to have the knowledge and tools necessary to provide nutrition recommendations and counseling to improve chronic disease management. A growing number of medical schools have begun to incorporate culinary medicine, an evidence-based discipline that offers an experiential learning approach to improve student's education in nutrition and address food-related social determinants of health.
Methods: In the fall of 2023, a culinary medicine pilot program was implemented for first-year medical students at the Larner College of Medicine (LCOM), aimed at increasing their nutrition knowledge and counseling skills. The course was led and developed by two second-year medical students certified in dietetics and integrative health with oversight provided by faculty physicians board-certified in family medicine and lifestyle medicine. The program included five sessions, each focusing on a different chronic disease. Each session consisted of a 45-min didactic lesson followed by a 45-min culinary medicine experiential lesson. The program took place in medical education classrooms utilizing small appliances and low-cost ingredients. The pilot program was evaluated by a post-program survey, which measured perceived knowledge, confidence, and intention to apply learning in clinical practice and personal life.
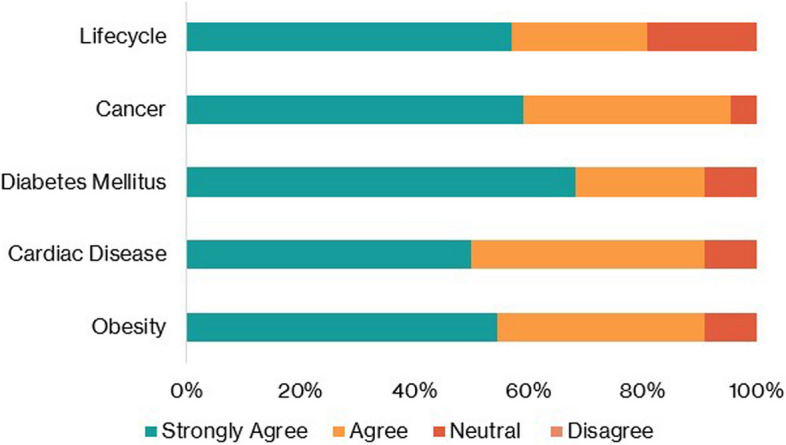
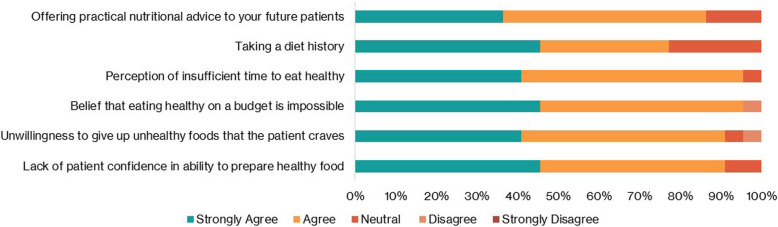
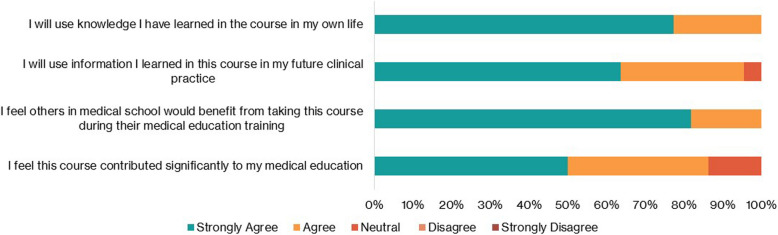
Results: The program included 26 first year medical students. The post-program survey revealed that 86% of respondents agreed they would use the information learned in the course in their future clinical practice, and 100% agreed they would apply this knowledge in their own lives. Ninety-one percent reported an enhanced understanding of the relationship between diet and disease, and 95% indicated increased confidence in providing nutrition counseling, particularly regarding social determinants of health.
Conclusion: These results demonstrate the benefits of a low-cost educational model of culinary medicine. Its potential to increase future physicians'nutrition knowledge and improve their confidence in providing meaningful, evidence-based dietary guidance is considerable.
Keywords: Culinary Medicine; Medical Education; Nutrition.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was determined to be exempt by the University of Vermont’s Institutional Review Board (STUDY00002825). Informed consent was obtained from all subjects prior to their participation. The study adhered to the guidelines put forth by the Helsinki Declaration. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
A Culinary Medicine Elective for Clinically Experienced Medical Students: A Pilot Study.J Altern Complement Med. 2020 Jul;26(7):636-644. doi: 10.1089/acm.2020.0063. Epub 2020 Jun 12. J Altern Complement Med. 2020. PMID: 32543207
-
Increasing nutrition knowledge and culinary skills in interprofessional healthcare students: an active learning pilot study.BMC Med Educ. 2025 May 26;25(1):777. doi: 10.1186/s12909-025-07247-y. BMC Med Educ. 2025. PMID: 40420132 Free PMC article.
-
Culinary medicine course: qualitative assessment of an innovative pedagogical approach.Public Health Nutr. 2025 Jun 30;28(1):e114. doi: 10.1017/S1368980025100414. Public Health Nutr. 2025. PMID: 40583367
-
Exploring culinary medicine as a promising method of nutritional education in medical school: a scoping review.BMC Med Educ. 2022 Jun 7;22(1):441. doi: 10.1186/s12909-022-03449-w. BMC Med Educ. 2022. PMID: 35672843 Free PMC article.
-
Important Nutritional Concepts and Recommendations at the Level of Medical School Education.Curr Nutr Rep. 2025 Apr 9;14(1):59. doi: 10.1007/s13668-025-00648-x. Curr Nutr Rep. 2025. PMID: 40202556 Review.
References
-
- Ahmed NU, Delgado M, Saxena A. Trends and disparities inthe prevalence of physicians’ counseling on diet and nutrition among the U.S. adult population, 2000–2011. Prev Med. 2016;89:70–5. - PubMed
-
- Birkhead AG, Foote S, Monlezun DJ, et al. Medical student-led community cooking classes: a novel preventive medicine model that’s easy to swallow. Am J Prev Med. 2014;46:e41–2. 10.1016/j.amepre.2013.11.006. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
