

Impact of an oral care intervention protocol on oral health outcomes in head and neck cancer patients undergoing radiation or chemoradiation therapy
- PMID: 40217239
- PMCID: PMC11987221
- DOI: 10.1186/s12903-025-05877-8
Impact of an oral care intervention protocol on oral health outcomes in head and neck cancer patients undergoing radiation or chemoradiation therapy
Abstract
Background: Head and neck cancer patients receiving chemotherapy and radiation therapy may experience a notable and frequently sudden decline in their oral health. These alterations include oral mucositis that develops during and shortly after treatment, candida infections, trouble speaking, difficulty eating, bleeding gums, and tissue fibrosis.
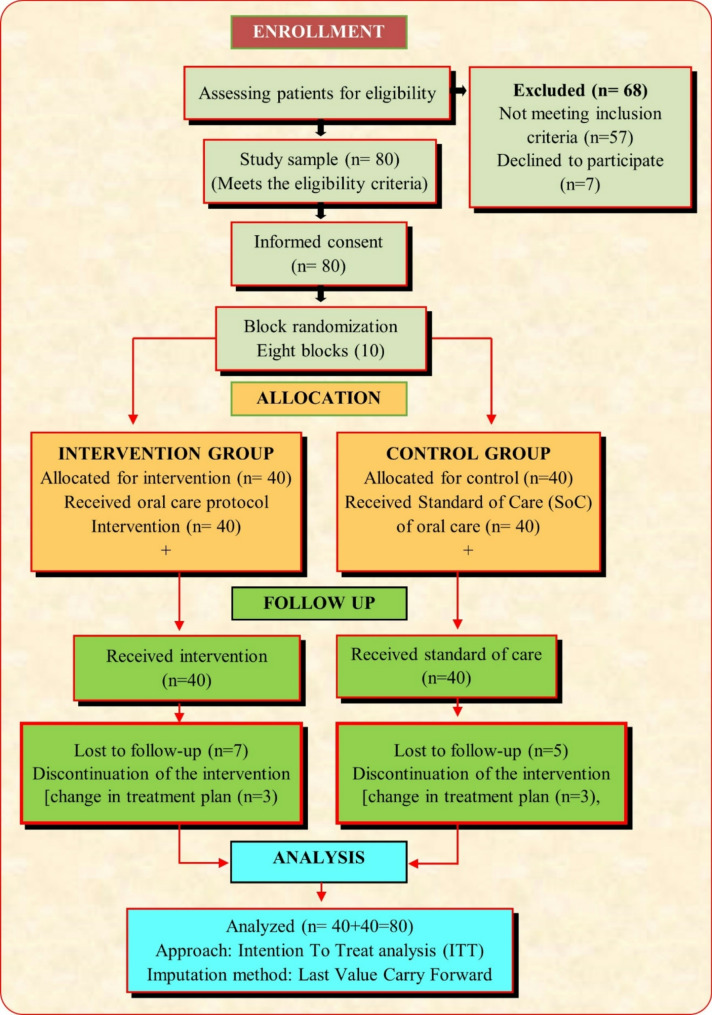
Materials and methods: This study aimed to determine the effectiveness of oral care intervention protocol (OCIP) on oral health and oral complications. The experimental group received a structured oral care protocol, and the control group received oral care as per the standard of care of the study setting. These patients were observed every week for up to 6 weeks until the completion of radiation therapy/chemoradiation. An experimental design using a randomized controlled trial was adopted for the study. After providing informed consent, the data were collected from 80 head and neck cancer patients.
Results: The maximum number of patients, i.e., 42.5% in the experimental group and 32.5% in the control group, were diagnosed with tongue cancer. Most of the participants, i.e., 57.5% in the experimental group and 67.5% in the control group, received chemoradiation as the treatment plan. Among all the oral complications, the median days to develop mucositis (p =.015), swallowing difficulty (p =.009), and chewing difficulty (p =.032) were significantly different from those of the control, indicating that the intervention was effective. As treatment progressed over the weeks, the severity of the oral problems increased in both groups (p =.001). Compared with routine care, oral care intervention improved oral health scores among cancer patients receiving head and neck radiation therapy/chemoradiation [F (401.982), p =.001].
Conclusion: These data suggest that the OCIP is clinically helpful in maintaining overall oral health among cancer patients receiving head and neck radiation/chemoradiation. The OCIP effectively delays the incidence of oral complications arising from head and neck radiation therapy/chemotherapy but does not prevent them. The findings of this study can also contribute to providing evidence for the use of an oral care kit, including all evidence-based interventions for patients receiving head and neck radiation/chemoradiation.
Keywords: Chemoradiation; Head and neck cancer patients; Oral care intervention protocol; Oral health outcomes; Radiation therapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Approval for this study was obtained in accordance with the Declaration of Helsinki from the ethics committee at the Institutional Ethics Committee of Kasturba Medical College, Mangalore (IEC KMC MLR 03–18/65). The trial was registered at the Clinical Trial Registry of India (CTRI/2015/04/005709; registration date: 21/04/2015). All patients provided written informed consent before enrolment in the study. Consent for publication: Not applicable Competing interests: The authors declare no competing interests.
Figures

References
-
- Huang T-J, Mu P-F, Chen M-B, Florczak K. Prevention and treatment of oral mucositis among cancer patients in the hematology–oncology setting: a best practice implementation project. JBI Evid Implement. 2020;18(4):420–30. - PubMed
-
- Sroussi HY, Epstein JB, Bensadoun RJ, Saunders DP, Lalla RV, Migliorati CA, et al. Common oral complications of head and neck cancer radiation therapy: mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med. 2017;6(12):2918–31. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
