

Factors associated with postoperative recurrence in perforated colorectal cancer: unraveling the high recurrence rate of perforated colorectal cancer
- PMID: 40217242
- PMCID: PMC11987410
- DOI: 10.1186/s12957-025-03783-5
Factors associated with postoperative recurrence in perforated colorectal cancer: unraveling the high recurrence rate of perforated colorectal cancer
Abstract
Background: Perforated colorectal cancer exhibits a higher recurrence rate than non-perforated colorectal cancer; however, the reasons for this difference remain unclear. This study identifies factors affecting recurrence in patients with perforated colorectal cancer who underwent R0 surgery.
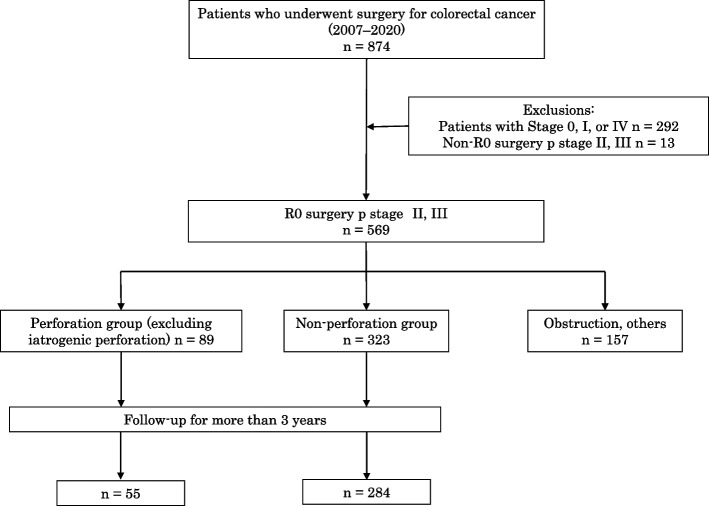
Methods: This study included consecutive patients with Stage II or III perforated colorectal cancer who underwent radical surgery at a single center between 2007 and 2020. The comparison group included patients with non-perforated, non-obstructive, non-perforated colorectal cancer who underwent surgery during the same period. Clinicopathological background factors (age, sex, localization, surgical procedure, stoma, T stage, lymphatic invasion, venous invasion, differentiation, extent of lymph node dissection, number of dissected lymph nodes, lymph node metastasis, postoperative complications, and 30-day postoperative death) of perforated and non-perforated colorectal cancers were investigated. Factors influencing recurrence were examined in patients who were followed for more than 3 years after surgery, up to 5 years postoperatively.
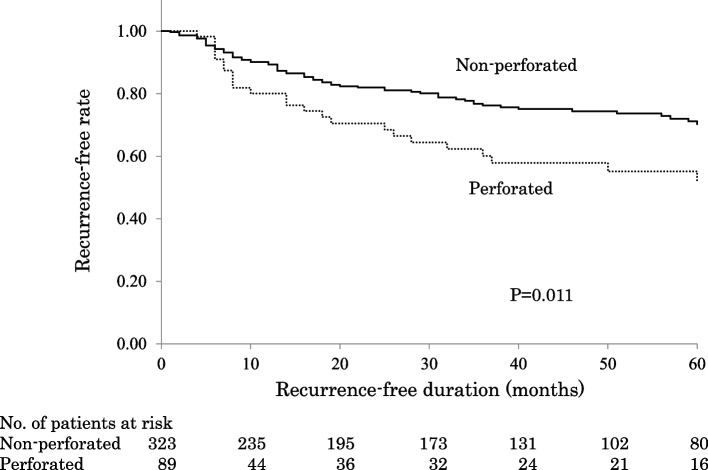
Results: This study included 89 perforated and 323 non-perforated cases. The median patient ages were 74 and 73 years in the perforated and non-perforated groups, respectively. In perforated cases, the proportion of T4 stage tumors was significantly higher (39% vs. 18% in non-perforated cases, with p < 0.001). Additionally, the number of lymph node dissections was significantly lower (10 vs. 17 in non-perforated cases, p < 0.001), and the rate of postoperative complications was higher (46% vs. 7% in the non-perforated cases, p < 0.001). Postoperatively, 55 perforated and 284 non-perforated cases were available for follow-up. Univariate analysis revealed that perforation, T4 stage, lymph node metastases, and postoperative complications were associated with significantly higher recurrence rates. Multivariate analysis identified T4 stage and lymph node metastases as independent risk factors.
Conclusions: The recurrence rate of perforated colorectal cancer was higher than that of non-perforated cases, primarily due to advanced disease stages, such as T4 or lymph node metastases. Perforation itself may not directly cause recurrence but reflects cancer progression. Further research is needed to clarify the mechanisms linking cancer progression, perforation, and recurrence.
Keywords: Colorectal neoplasms; Intestinal perforation; Neoplasm staging.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures involving human participants performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Institutional Review Board of Saitama Medical University Hospital (No. 19071), which waived the requirement for written informed consent from the participants owing to its retrospective design. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Risk factors for the recurrence of stage II perforated colorectal cancer: A retrospective observational study.Asian J Surg. 2023 Jan;46(1):201-206. doi: 10.1016/j.asjsur.2022.03.026. Epub 2022 Mar 21. Asian J Surg. 2023. PMID: 35331590
-
Risk Factors and Patterns of Recurrence in Stage III Perforated Colorectal Cancer: A Single-Center, Retrospective, Observational Study.Cureus. 2025 Jan 14;17(1):e77446. doi: 10.7759/cureus.77446. eCollection 2025 Jan. Cureus. 2025. PMID: 39958103 Free PMC article.
-
Postoperative recurrence and risk factors of colorectal cancer perforation.Int J Colorectal Dis. 2017 Mar;32(3):419-424. doi: 10.1007/s00384-016-2694-3. Epub 2016 Oct 30. Int J Colorectal Dis. 2017. PMID: 27796497
-
Emergency surgery for obstructing and perforated colon cancer: patterns of recurrence and prognostic factors.Tech Coloproctol. 2019 Dec;23(12):1141-1161. doi: 10.1007/s10151-019-02110-x. Epub 2019 Nov 14. Tech Coloproctol. 2019. PMID: 31728784
-
Metastatic lymphs nodes and lymph node ratio as predictive factors of survival in perforated and non-perforated T4 colorectal tumors.J Surg Oncol. 2013 Sep;108(3):176-81. doi: 10.1002/jso.23373. Epub 2013 Jul 7. J Surg Oncol. 2013. PMID: 23832524
References
-
- Kriwanek S, Armbruster C, Beckerhinn P, Ditrich K. Prognostic factors for survival in colonic perforation. Int J Colorectal Dis. 1994;9:158–62. - PubMed
-
- Bielecki K, Kamiński P, Klukowski M. Large bowel perforation: morbidity and mortality. Tech Coloproctol. 2002;6:177–82. - PubMed
-
- Biondo S, Parés D, Martí Ragué J, De Oca J, Toral D, Borobia FG, et al. Emergency operations for nondiverticular perforation of the left colon. Am J Surg. 2002;183:256–60. - PubMed
-
- Biondo S, Ramos E, Deiros M, Ragué JM, De Oca J, Moreno P, et al. Prognostic factors for mortality in left colonic peritonitis: a new scoring system. J Am Coll Surg. 2000;191:635–42. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
