

De novo ADGRV1 variant in a patient with ictal asystole provides novel clues for increased risk of SUDEP
- PMID: 40217298
- PMCID: PMC11960348
- DOI: 10.1186/s42494-023-00124-5
De novo ADGRV1 variant in a patient with ictal asystole provides novel clues for increased risk of SUDEP
Abstract
Background: Various cardiac and autonomic manifestations are frequently reported during seizures. Among the seizure-related arrhythmia, ictal tachycardia is the most common, followed by ictal bradycardia, with ictal asystole being the rarest. The occurrence of ictal asystole may obscure the clinical presentation and delay the diagnosis, representing a life-threatening presentation of epilepsy, with an elevated risk of sudden unexpected death in epilepsy patients (SUDEP). These cardiac abnormalities are being increasingly recognized as the key to elucidating the mechanisms of SUDEP.
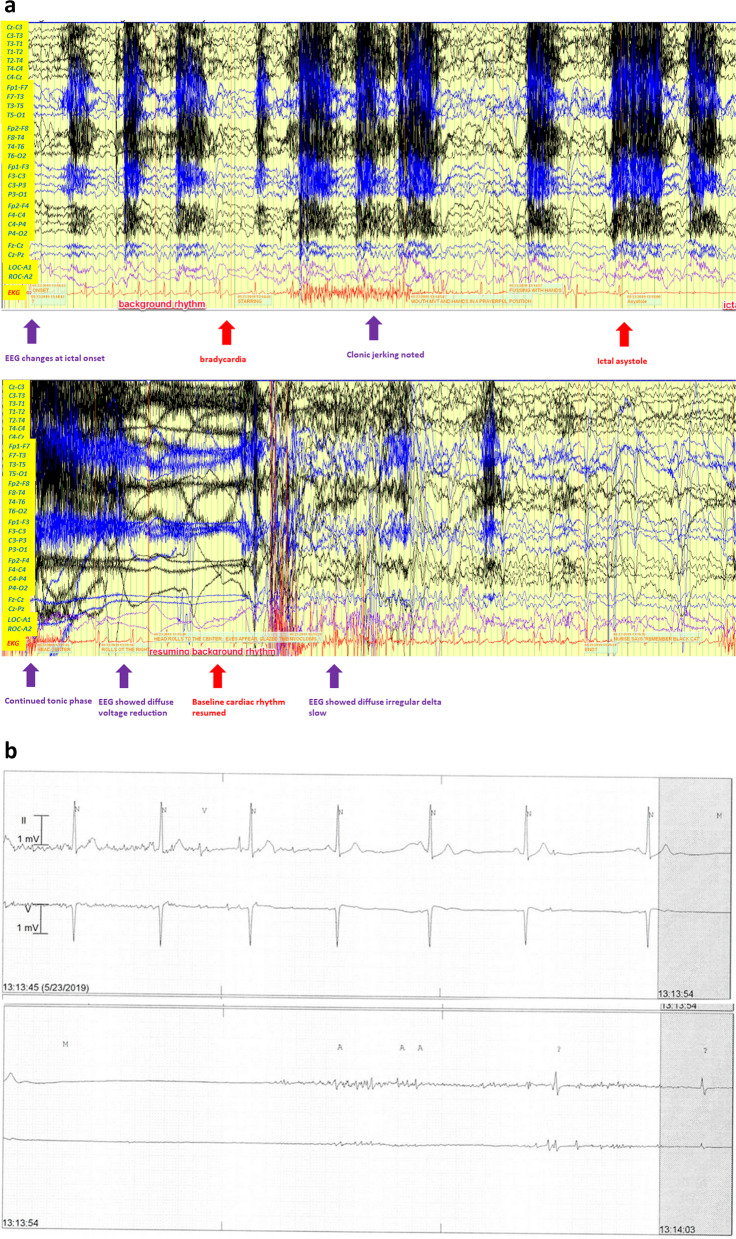
Case presentation: We present a 35-year-old man with a history of focal-onset seizures with impaired consciousness since his mid-20 s. He developed different types of seizures for 2 years, described as tonic seizure and atonic seizure (drop attack). During such clinical events, he suffered from falls and cardiac arrest. However, thorough cardiac electrophysiology and imaging workup failed to reveal a cardiac etiology. Subsequent video electroencephalograph (EEG) monitoring was performed, and ictal bradycardia and ictal asystole were discovered. A cardiac pacemaker was implanted, and at 3-year follow-up, the patient did not suffer more atonic seizures, or falls. Genetic tests discovered a de novo variant of Adhesion G Protein-Coupled Receptor V1 (ADGRV1), which may provide a clue for the patient's ictal asystole and the increased risk of SUDEP.
Conclusions: Considering the important impact of ictal bradycardia and asystole on the morbidity and potential mortality of epileptic patients, it is important to simultaneously utilize EEG and electrocardiogram to confirm the diagnosis. This case report highlights the link between the de novo variant of ADGRV1 and the ictal bradycardia/asystole phenotype and implicates the importance of genetic testing in adult epilepsy patients.
Keywords: ADGRV1; Drug resistant epilepsy; Ictal asystole; SUDEP.
© 2023. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Institutional Ethics Committee of Kaiser Permanente Foundation Hospital (KPSAC 131–21) and written informed consent has been obtained from the patient. Consent for publication: Written informed consent for publication was obtained from the patient. Competing interests: The authors declare that they have no competing interests.
Figures


Similar articles
-
Ictal asystole: a case presentation.BMC Neurol. 2018 Jul 21;18(1):100. doi: 10.1186/s12883-018-1105-5. BMC Neurol. 2018. PMID: 30031379 Free PMC article.
-
Ictal bradyarrhythmias and asystole requiring pacemaker implantation: Combined EEG-ECG analysis of 5 cases.Epilepsy Behav. 2016 Nov;64(Pt A):212-215. doi: 10.1016/j.yebeh.2016.06.026. Epub 2016 Oct 14. Epilepsy Behav. 2016. PMID: 27750160
-
Comparison of clinical and electrophysiological characteristics between ictal and cardiac asystole encountered during video-EEG monitoring.Epileptic Disord. 2019 Aug 1;21(4):337-346. doi: 10.1684/epd.2019.1085. Epileptic Disord. 2019. PMID: 31371275
-
Syncope, Epilepsy and Ictal Asystole: A Case Series and Narrative Review.Heart Lung Circ. 2022 Jan;31(1):25-31. doi: 10.1016/j.hlc.2021.07.003. Epub 2021 Aug 6. Heart Lung Circ. 2022. PMID: 34366218 Review.
-
Cardiac arrhythmias during or after epileptic seizures.J Neurol Neurosurg Psychiatry. 2016 Jan;87(1):69-74. doi: 10.1136/jnnp-2015-310559. Epub 2015 Jun 2. J Neurol Neurosurg Psychiatry. 2016. PMID: 26038597 Free PMC article. Review.
References
-
- Tenyi D, Gyimesi C, Kupo P, Horvath R, Bone B, Barsi P, et al. Ictal asystole: A systemic review. Epilepsia. 2017;58:356–62. - PubMed
-
- Schuele SU, Widdess-Walsh P, Bermeo A, Lüders HO. Sudden unexplained death in epilepsy: the role of the heart. Cleve Clin J Med. 2007;74(Suppl 1):S121–7. - PubMed
-
- Leung H, Kwan P, Elger CE. Finding the missing link between ictal bradyarrhythmia, ictal asystole, and sudden unexpected death in epilepsy. Epilepsy Behav. 2006;9(1):19–30. - PubMed
LinkOut - more resources
Full Text Sources