

Status epilepticus in patients with genetic generalized epilepsy: a case series study
- PMID: 40217404
- PMCID: PMC11960239
- DOI: 10.1186/s42494-023-00144-1
Status epilepticus in patients with genetic generalized epilepsy: a case series study
Abstract
Background: Genetic generalized epilepsy (GGE) accounts for nearly one-third of all epilepsies. The feature of status epilepticus (SE) in patients with GGE has been rarely studied. We aimed to determine the electroclinical characteristics of SE in patients with GGE.
Methods: In this retrospective study, nine patients with GGE were enrolled at Xijing Hospital, Xi'an, China from May 2014 to May 2020. SE was confirmed by 24-h video-EEG recording. The demography, clinical manifestation, brain MRI and SE pattern were analyzed.
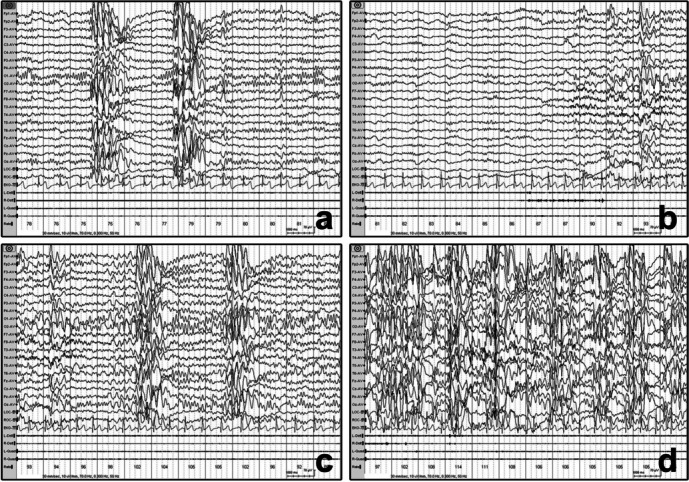
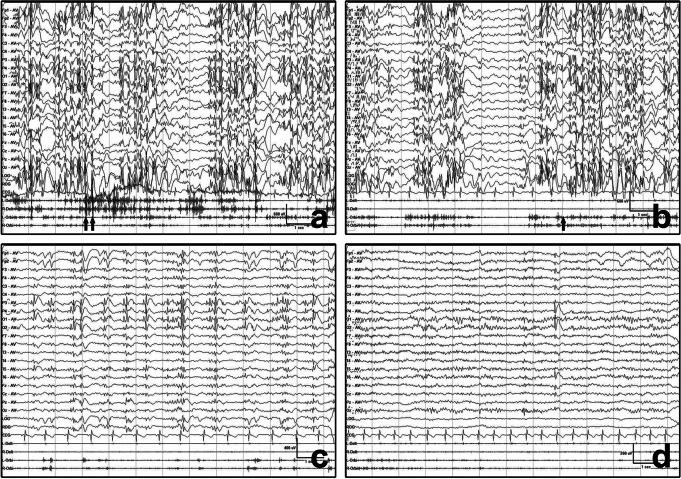
Results: Of the nine patients in the study, seven were female. The mean age of the patients at the time of inclusion was 16.8 years (range 7-31 years), and the mean age at the onset of epilepsy was 10.9 years (range 6-17 years). The follow-up time ranged from 3 months to 6 years. Myoclonic absence status was identified in four patients showing eyelid myoclonia with absence and one patient showing perioral myoclonia with absences. Myoclonic SE was identified in three patients showing juvenile myoclonic epilepsy. Autonomic SE was found in one patient with eyelid myoclonia with absence. SE was terminated by oral midazolam in four patients. In the other five patients, SE terminated spontaneously.
Conclusions: The seizure type of SE in patients with GGE is often consistent with their major symptoms. Oral midazolam may be an option to terminate SE in patients with GGE.
Keywords: Electroencephalography; Genetic generalized epilepsy; Status epilepticus.
© 2023. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This report was approved by the Medical Ethics Committee of the First Affiliated Hospital of the Air Force Mdical University (KY20222046-C-1), and patients or their guardians signed informed consent. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines. Consent for publication: All participants gave consent for publication. Competing interests: All authors disclose that they have no conflicts of interest.
Figures
Similar articles
-
Generalized Fast Discharges Along the Genetic Generalized Epilepsy Spectrum: Clinical and Prognostic Significance.Front Neurol. 2022 Mar 10;13:844674. doi: 10.3389/fneur.2022.844674. eCollection 2022. Front Neurol. 2022. PMID: 35356452 Free PMC article.
-
Unmasking the entity of 'drug-resistant' perioral myoclonia with absences: the twitches, darts and domes!Epileptic Disord. 2021 Apr 1;23(2):313-324. doi: 10.1684/epd.2021.1265. Epileptic Disord. 2021. PMID: 33851919
-
Jeavons syndrome in China.Epilepsy Behav. 2014 Mar;32:64-71. doi: 10.1016/j.yebeh.2013.12.016. Epub 2014 Feb 1. Epilepsy Behav. 2014. PMID: 24495864
-
Modified Atkins diet in children with epilepsy with eyelid myoclonia (Jeavons syndrome).Epilepsy Behav. 2023 Aug;145:109347. doi: 10.1016/j.yebeh.2023.109347. Epub 2023 Jul 16. Epilepsy Behav. 2023. PMID: 37459720 Review.
-
Status epilepticus in idiopathic generalized epilepsy.Epilepsia. 2005;46 Suppl 9:73-9. doi: 10.1111/j.1528-1167.2005.00316.x. Epilepsia. 2005. PMID: 16302878 Review.
References
-
- Betjemann JP, Lowenstein DH. Status epilepticus in adults. Lancet Neurol. 2015;14:615–24. - PubMed
-
- Yasam VR, Senthil V, Jakki SL, Jawahar N. Status epilepticus: an overview. Curr Drug Metab. 2017;18:174–85. - PubMed
-
- Trinka E, Cock H, Hesdorffer D, Rossetti AO, Scheffer IE, Shinnar S, et al. A definition and classification of status epilepticus–report of the ILAE task force on classification of status epilepticus. Epilepsia. 2015;56(10):1515–23. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources