

Reversible leukoencephalopathy with seizures: a case of severe high-altitude cerebral edema
- PMID: 40217406
- PMCID: PMC11960260
- DOI: 10.1186/s42494-024-00165-4
Reversible leukoencephalopathy with seizures: a case of severe high-altitude cerebral edema
Abstract
Background: Acute high-altitude illness (AHAI) refers to a series of syndromes including acute mountain sickness (AMS), high-altitude pulmonary edema (HAPE) and high-altitude cerebral edema (HACE). Among these, HACE is a severe and potentially life-threatening condition that can occur when individuals ascend to high altitudes. It is often characterized by ataxia, confusion, and altered mental status. Without appropriate treatment, HACE can rapidly progress to coma, but seizures are infrequent in occurrence.
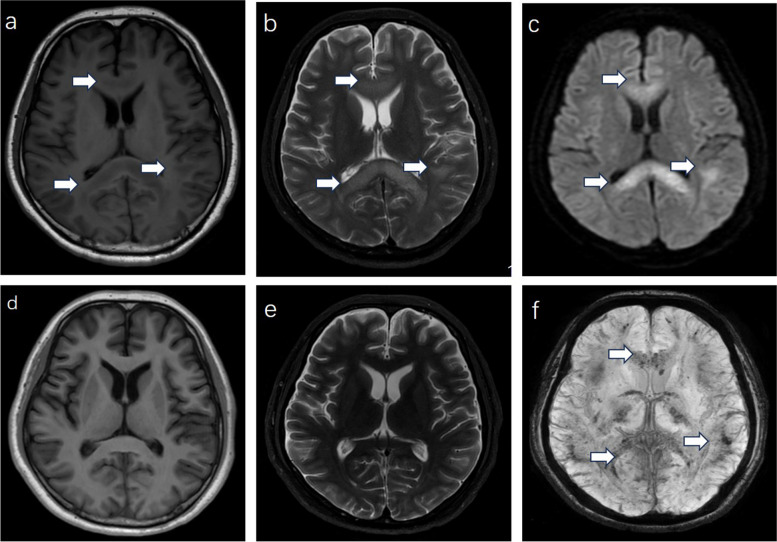
Case presentation: Here, we report a severe HACE patient with coma and status epilepticus. The patient is a 23-year-old male who was visiting Lhasa for the first time. He initially experienced headaches and dizziness on the first day, and then he was found in coma with limb convulsions on the next day. Immediate medical attention was sought, and brain CT and MRI scans showed reversible white matter lesions, especially in the corpus callosum and subcortical white matter. Although the lesions disappeared on T1 and T2 sequences, microbleeds were observed on the SWI sequence. After treatment with tracheal intubation, glucocorticoids and hyperbaric oxygen, the cerebral edema has resolved and the clinical symptoms improved, the patient has no seizures anymore.
Conclusions: HACE typically follows AMS and poses a significant risk to life. Clinical manifestations mainly include ataxia, alterations of behavior, and impaired consciousness, with severe cases progressing to coma. Seizures, though rarely observed, may occur. Imaging shows reversible white matter lesions, with microbleeds being a significant and persistent imaging marker over time. Administration of glucocorticoids plays a crucial role in treatment. Despite experiencing seizures, this patient did not experienced any further episodes once his condition improved.
Keywords: Case report; High-altitude cerebral edema; Microbleeds; Reversible leukoencephalopathy; Seizures.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Medical Ethics Committee of Sichuan University West China Hospital (Ethical approval number: 2023 [1428]) and informed consent was obtained from the patient and the patient’s parents. Consent for publication: Not applicable. Competing interests: The authors declare no conflict of interest in this manuscript.
Figures


Similar articles
-
Does Prior Respiratory Infection Increase the Risk of High-Altitude Pulmonary and Cerebral Edema? A Case Report.High Alt Med Biol. 2025 Jun 2. doi: 10.1089/ham.2025.0021. Online ahead of print. High Alt Med Biol. 2025. PMID: 40452580
-
Susceptibility - weighted imaging: A valuable diagnostic tool for early detection of high-altitude cerebral edema: A case report.Radiol Case Rep. 2023 Jun 22;18(9):3089-3092. doi: 10.1016/j.radcr.2023.06.009. eCollection 2023 Sep. Radiol Case Rep. 2023. PMID: 37434613 Free PMC article.
-
Study of high-altitude cerebral edema using multimodal imaging.Front Neurol. 2023 Jan 26;13:1041280. doi: 10.3389/fneur.2022.1041280. eCollection 2022. Front Neurol. 2023. PMID: 36776573 Free PMC article.
-
High altitude cerebral edema and acute mountain sickness. A pathophysiology update.Adv Exp Med Biol. 1999;474:23-45. doi: 10.1007/978-1-4615-4711-2_2. Adv Exp Med Biol. 1999. PMID: 10634991 Review.
-
High-altitude cerebral edema (HACE): the Denver/Front Range experience.Semin Neurol. 2000;20(2):209-17. doi: 10.1055/s-2000-9830. Semin Neurol. 2000. PMID: 10946741 Review.
References
-
- Hackett PH, Roach RC. High-altitude illness. N Engl J Med. 2001;345(2):107–14. - PubMed
-
- Basnyat B, Murdoch DR. High-altitude illness. Lancet. 2003;361(9373):1967–74. - PubMed
-
- Jensen JD, Vincent AL. High Altitude Cerebral Edema. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. PMID: 28613666. - PubMed
-
- Imray C, Booth A, Wright A, Bradwell A. Acute altitude illnesses. BMJ. 2011;343:d4943. - PubMed
-
- Luks AM, Auerbach PS, Freer L, Grissom CK, Keyes LE, McIntosh SE, et al. Wilderness medical society clinical practice guidelines for the prevention and treatment of acute altitude illness: 2019 update. Wilderness Environ Med. 2019;30(4S):S3-18. - PubMed
LinkOut - more resources
Full Text Sources