

Multimodal assessment of favorable neurological outcome using NSE levels and kinetics, EEG and SSEP in comatose patients after cardiac arrest
- PMID: 40217465
- PMCID: PMC11992829
- DOI: 10.1186/s13054-025-05378-8
Multimodal assessment of favorable neurological outcome using NSE levels and kinetics, EEG and SSEP in comatose patients after cardiac arrest
Abstract
Background: Prognostic markers of good neurological outcome after cardiac arrest (CA) remain limited. We aimed to evaluate the prognostic value of neuron-specific enolase (NSE), electroencephalogram (EEG) and somatosensory evoked potentials (SSEP) in predicting good outcome, assessed separately and in combination.
Methods: A retrospective study was conducted in a tertiary CA center, using a prospective registry. We included all patients comatose after discontinuation of sedation and with one EEG and NSE blood measurement at 24, 48 or/and 72 h after CA. The primary outcome was favorable neurological outcome at three months, a Cerebral Performance Categories (CPC) scale 1-2 defining a good outcome.
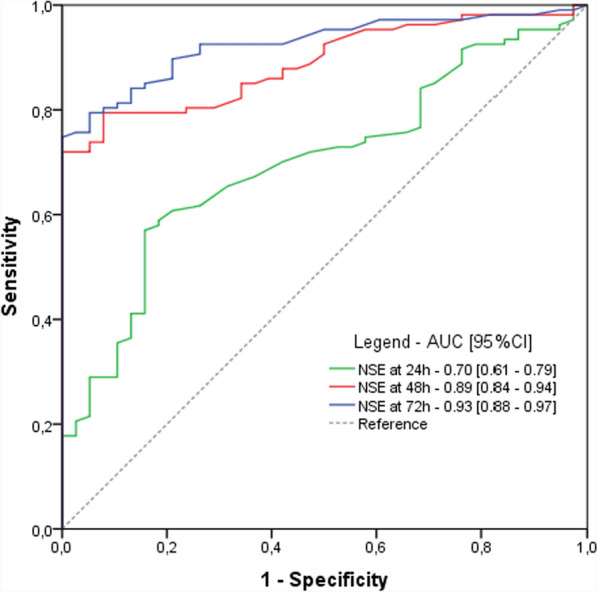
Results: Between January 2017 and April 2024, 215 patients were included. Participants were 63 years old (IQR [52-73]), and 73% were male. At 3 months, 54 patients (25.1%) had a good outcome. Compared to the poor outcome group, NSE blood levels were significantly lower in the good outcome group at 24 h (39 IQR[27-45] vs 54 IQR[37-82]µg/L, p < 0.001), 48 h (26 [18-43] vs 107 [54-227]µg/L, p < 0.001) and 72 h (20 µg/L IQR [15-30] vs 184 µg/l IQR [60-300], p < 0,001). Normal NSE (i.e., < 17 µg/L) at 24 h was highly predictive of good outcome, with a predictive positive value (PPV) of 71% despite a sensitivity (Se) of 9%. The best cut-off values for NSE at 24, 48 and 72 h were below 45.5, 51.5 and 41.5 µg/L, yielding PPV of 64%, 80% and 83% and sensitivities of 74%, 93% and 90%, respectively. A decreasing trend in NSE levels between 24 and 72 h was also highly predictive of good outcome (PPV 82%, Se 81%). A benign EEG pattern was more frequently observed in the good outcome group (87.1 vs 14.9%, p < 0.001) and predicted a good outcome with a PPV of 72% and a Se of 94%. Regarding SSEPs, a bilateral N20-baseline amplitude > 0.85 µV was predictive of good outcome (PPV 75%, Se 100%). The combination of NSE < 51.5 µg/l at 48 h, a decreasing NSE trend between 24 and 72 h and a benign EEG showed the best predictive value (PPV 96%, Se 76%).
Conclusion: In comatose patients after CA, a low NSE levels at 24, 48 h or 72 h, a decreasing trend in NSE over time, a benign EEG and a high N20 amplitude are robust markers of favorable outcome, reducing prognosis uncertainty.
Keywords: Cardiac arrest; Coma; EEG; Electroencephalography; NSE; Neuron-specific enolase; Neuroprognostication; SSEP; Somatosensory-evoked potentials.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The research protocol was approved by the ethical committees (2019-A01378-49, CPP-SMIV-190901; 2022-A01811 42; CPP-Ile-de-France-I) and the French data protection authorities, in accordance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Performance of the ERC/ESICM-recommendations for neuroprognostication after cardiac arrest: Insights from a prospective multicenter cohort.Resuscitation. 2024 Sep;202:110362. doi: 10.1016/j.resuscitation.2024.110362. Epub 2024 Aug 14. Resuscitation. 2024. PMID: 39151721
-
SSEP N20 and P25 amplitudes predict poor and good neurologic outcomes after cardiac arrest.Ann Intensive Care. 2022 Mar 15;12(1):25. doi: 10.1186/s13613-022-00999-6. Ann Intensive Care. 2022. PMID: 35290522 Free PMC article.
-
Serum neuron-specific enolase as predictor of outcome in comatose cardiac-arrest survivors: a prospective cohort study.BMC Cardiovasc Disord. 2011 Aug 8;11:48. doi: 10.1186/1471-2261-11-48. BMC Cardiovasc Disord. 2011. PMID: 21824428 Free PMC article.
-
Biochemical markers and somatosensory evoked potentials in patients after cardiac arrest: the role of neurological outcome scores.J Neurol Sci. 2011 Jun 15;305(1-2):80-4. doi: 10.1016/j.jns.2011.03.007. Epub 2011 Mar 26. J Neurol Sci. 2011. PMID: 21440912 Review.
-
Prediction of good neurological outcome in comatose survivors of cardiac arrest: a systematic review.Intensive Care Med. 2022 Apr;48(4):389-413. doi: 10.1007/s00134-022-06618-z. Epub 2022 Mar 4. Intensive Care Med. 2022. PMID: 35244745 Free PMC article.
Cited by
-
Absolute blood levels and kinetics of neurofilament light (NFL) chains for neurological prognosis in comatose patients after cardiac arrest.Ann Intensive Care. 2025 May 30;15(1):75. doi: 10.1186/s13613-025-01491-7. Ann Intensive Care. 2025. PMID: 40445422 Free PMC article.
References
-
- Cronberg T, Greer DM, Lilja G, Moulaert V, Swindell P, Rossetti AO. Brain injury after cardiac arrest: from prognostication of comatose patients to rehabilitation. Lancet Neurol. 2020;19(7):611–22. - PubMed
-
- Perkins GD, Callaway CW, Haywood K, Neumar RW, Lilja G, Rowland MJ, et al. Brain injury after cardiac arrest. The Lancet. 2021;398(10307):1269–78. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
