

The Effectiveness of an Electronic Decision Support Algorithm to Optimize Recommendations of SGLT2i and GLP-1RA in Patients with Type 2 Diabetes upon Discharge from Internal Medicine Wards
- PMID: 40217621
- PMCID: PMC11989524
- DOI: 10.3390/jcm14072170
The Effectiveness of an Electronic Decision Support Algorithm to Optimize Recommendations of SGLT2i and GLP-1RA in Patients with Type 2 Diabetes upon Discharge from Internal Medicine Wards
Abstract
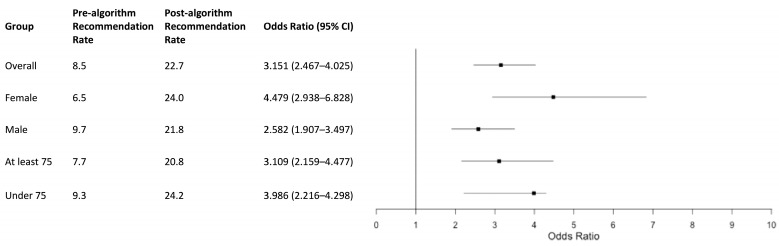
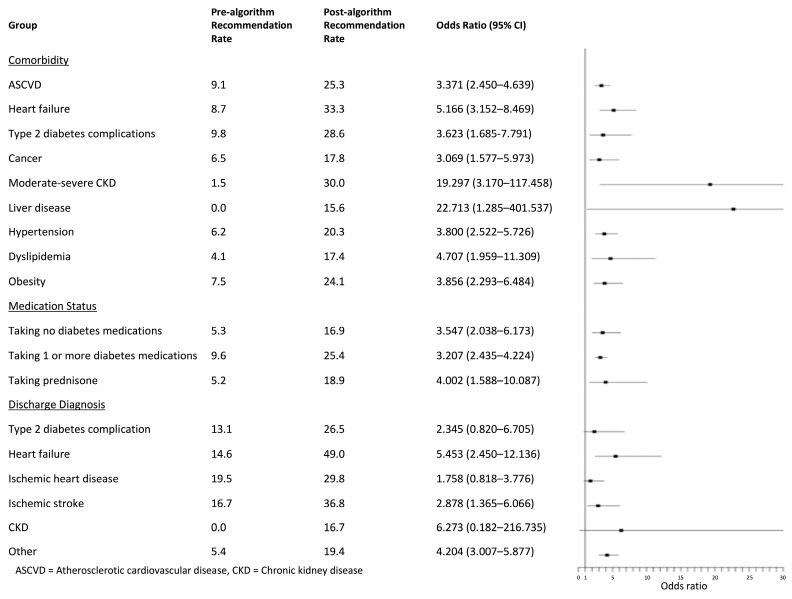
Background/Objectives: Despite the established cardiovascular benefit of sodium-glucose cotransporter-2 inhibitors (SGLT2is) and glucagon-like peptide-1 receptor agonists (GLP-1RAs), these medications are under-prescribed in patients with type 2 diabetes. Our study aims to examine the effectiveness of a clinical decision support system (CDSS) in improving the recommendation rate of SGLT2i and GLP-1RA upon discharge. Methods: We developed an algorithm to automatically recommend SGLT2is and GLP-1RAs for eligible patients with type 2 diabetes upon discharge, based on current guidelines. Data were collected from electronic medical records of all eligible patients ≥18 years old hospitalized in one of five internal medicine wards at Beilinson Hospital. The primary outcome was to evaluate the rate of physician recommendation of SGLT2is and GLP-1RAs at discharge, before and after algorithm implementation. Results: Our study included 1318 patients in the pre-algorithm group and 970 in the post-algorithm group. The recommendation rate of SGLT2is and GLP-1RAs was 8.5% in the pre-algorithm group and 22.7% in the post-algorithm. The odds ratio (OR) of recommendation in the post- vs. pre-algorithm group was 3.151 (95% CI: 2.467-4.025, p < 0.0001). Recommendation rates increased in all subgroups analyzed, notably in patients hospitalized due to heart failure (recommendation rate pre-algorithm: 14.6% vs. post-algorithm: 49.02%). Conclusions: This study demonstrates the benefit of a CDSS in improving the recommendation rate of SGLT2is and GLP-1RAs in patients with type 2 diabetes upon discharge from hospitalization. Future studies should assess the impact of the algorithm on recommendation rates in other wards, medication utilization, and long-term outcomes.
Keywords: GLP-1RA; SGLT2i; clinical decision support system; electronic decision support algorithm; type 2 diabetes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
National Trends in Use of Sodium-Glucose Cotransporter-2 Inhibitors and Glucagon-like Peptide-1 Receptor Agonists by Cardiologists and Other Specialties, 2015 to 2020.J Am Heart Assoc. 2022 May 3;11(9):e023811. doi: 10.1161/JAHA.121.023811. Epub 2022 Apr 27. J Am Heart Assoc. 2022. PMID: 35475341 Free PMC article.
-
Combining glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter-2 inhibitors (SGLT2is) in patients with type 2 diabetes mellitus (T2DM).Cardiovasc Diabetol. 2023 Apr 1;22(1):79. doi: 10.1186/s12933-023-01798-4. Cardiovasc Diabetol. 2023. PMID: 37005640 Free PMC article. Review.
-
Association between glucagon-like peptide-1 receptor agonists and biliary-related diseases in patients with type 2 diabetes: A nationwide cohort study.Pharmacotherapy. 2022 Jun;42(6):483-494. doi: 10.1002/phar.2688. Epub 2022 May 17. Pharmacotherapy. 2022. PMID: 35508702
-
Real-world effectiveness of adding newer generation GLP-1RA to SGLT2i in type 2 diabetes.Cardiovasc Diabetol. 2025 Apr 24;24(1):177. doi: 10.1186/s12933-025-02737-1. Cardiovasc Diabetol. 2025. PMID: 40275332 Free PMC article.
-
Real-world evidence on the utilization, clinical and comparative effectiveness, and adverse effects of newer GLP-1RA-based weight-loss therapies.Diabetes Obes Metab. 2025 Apr;27 Suppl 2(Suppl 2):66-88. doi: 10.1111/dom.16364. Epub 2025 Apr 8. Diabetes Obes Metab. 2025. PMID: 40196933 Free PMC article. Review.
References
-
- Ong K.L., Stafford L.K., McLaughlin S.A., Boyko E.J., Vollset S.E., Smith A.E., Dalton B.E., Duprey J., Cruz J.A., Hagins H., et al. Global, Regional, and National Burden of Diabetes from 1990 to 2021, with Projections of Prevalence to 2050: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402:203–234. doi: 10.1016/S0140-6736(23)01301-6. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
