

Prevalence of Temporal Lobe Epilepsy (TLE) Subtypes and Response to Resective Surgery in Patients with Presumed TLE Undergoing Limbic and Paralimbic Network Exploration with Stereo-Electrodes
- PMID: 40217635
- PMCID: PMC11989876
- DOI: 10.3390/jcm14072184
Prevalence of Temporal Lobe Epilepsy (TLE) Subtypes and Response to Resective Surgery in Patients with Presumed TLE Undergoing Limbic and Paralimbic Network Exploration with Stereo-Electrodes
Abstract
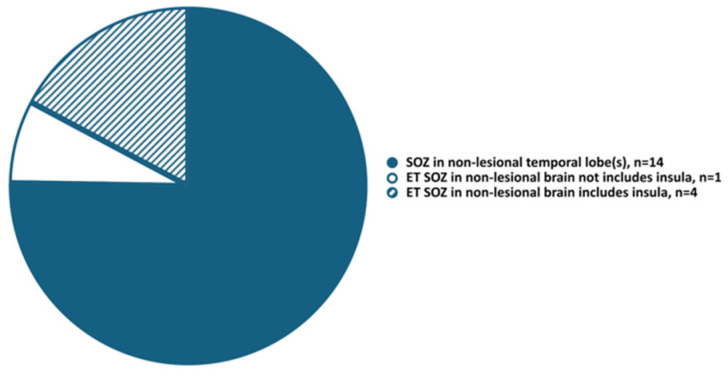
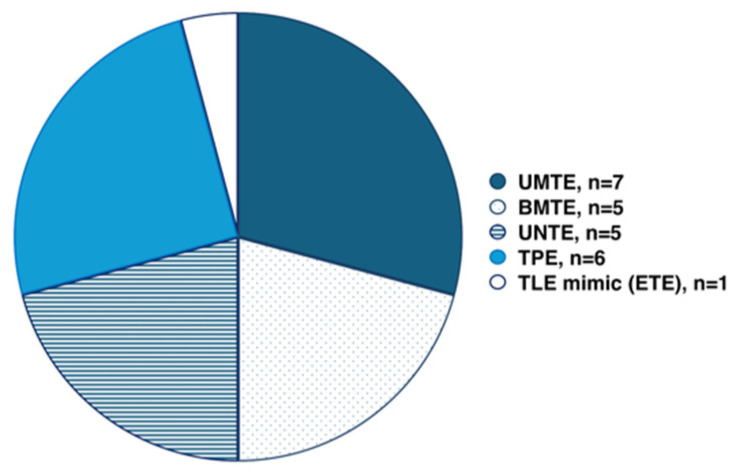
Background/Objectives: Temporal lobe epilepsy (TLE) responds well to surgical treatment, although a considerable percentage of patients experience seizure recurrence after resection. Relapse from the contralateral mesial temporal lobe, extratemporal lobe epilepsy mimicking TLE, or temporal plus epilepsy might account for surgical failures. Methods: We included patients with a pre-implantation hypothesis suggesting TLE, who underwent stereo-EEG (SEEG) evaluation at our institution and had an individual SEEG exploration paradigm with at least twelve stereo-electrodes placed to sixteen brain regions allowing exploration of limbic and paralimbic networks. We analyzed the prevalence of TLE subtypes based on ictal onset localization with SEEG and response to resective surgery. Results: Twenty-four subjects met the inclusion criteria. Seven patients had unilateral mesial temporal epilepsy (UMTE), five had bilateral mesial temporal epilepsy (BMTE), five had unilateral neocortical temporal epilepsy (UNTE), six had temporal-plus epilepsy (TPE), one had extratemporal epilepsy (ETE). The number of patients who underwent destructive surgeries and surgical outcomes are as follows: UMTE-all seven patients, Engel I; BMTE- three out of five, Engel I, III, and IV, respectively; UNTE-three out of five, Engel I; TLE mimic (ETE)-one, Engel I; TPE-all six patients, Engel I-three, Engel III-two, Engel IV-one. Conclusions: In our study, UMTE was the most frequent TLE subtype (29%), and all patients proceeded to resective surgery with good outcomes. TPE comprised a substantial component (25%) of this cohort with initially presumed TLE, who had a notable proportion of unfavorable outcomes. Larger studies are needed to create guidelines for rational counseling of patients with presumed TLE regarding surgical outcomes.
Keywords: epilepsy surgery; strereoelectroencephalography (SEEG); temporal lobe epilepsy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Exploration of epileptic networks in temporal lobe encephaloceles with stereotactic EEG: Electroclinical characteristics and surgical outcomes.Epilepsia Open. 2024 Dec;9(6):2395-2407. doi: 10.1002/epi4.13063. Epub 2024 Oct 7. Epilepsia Open. 2024. PMID: 39374038 Free PMC article.
-
Temporal lobe epilepsy in patients with nonlesional MRI and normal memory: an SEEG study.J Neurosurg. 2015 Dec;123(6):1368-74. doi: 10.3171/2015.1.JNS141811. Epub 2015 Jul 24. J Neurosurg. 2015. PMID: 26207602
-
Seizure semiology in temporal lobe vs. temporal plus epilepsy using intracranial EEG monitoring.Neurosciences (Riyadh). 2021 Jul;26(3):261-269. doi: 10.17712/nsj.2021.3.20200156. Neurosciences (Riyadh). 2021. PMID: 34230081 Free PMC article.
-
Surgical outcomes related to invasive EEG monitoring with subdural grids or depth electrodes in adults: A systematic review and meta-analysis.Seizure. 2019 Aug;70:12-19. doi: 10.1016/j.seizure.2019.06.022. Epub 2019 Jun 18. Seizure. 2019. PMID: 31234050
-
Surgery procedures in temporal lobe epilepsies.Handb Clin Neurol. 2022;187:531-556. doi: 10.1016/B978-0-12-823493-8.00007-9. Handb Clin Neurol. 2022. PMID: 35964991 Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
