

Biomarkers Affecting Treatment Outcomes of Febrile Neutropenia in Hematological Patients with Lymphomas: Is Presepsin the New Promising Diagnostic and Prognostic Biomarker?
- PMID: 40217689
- PMCID: PMC11989253
- DOI: 10.3390/jcm14072238
Biomarkers Affecting Treatment Outcomes of Febrile Neutropenia in Hematological Patients with Lymphomas: Is Presepsin the New Promising Diagnostic and Prognostic Biomarker?
Abstract
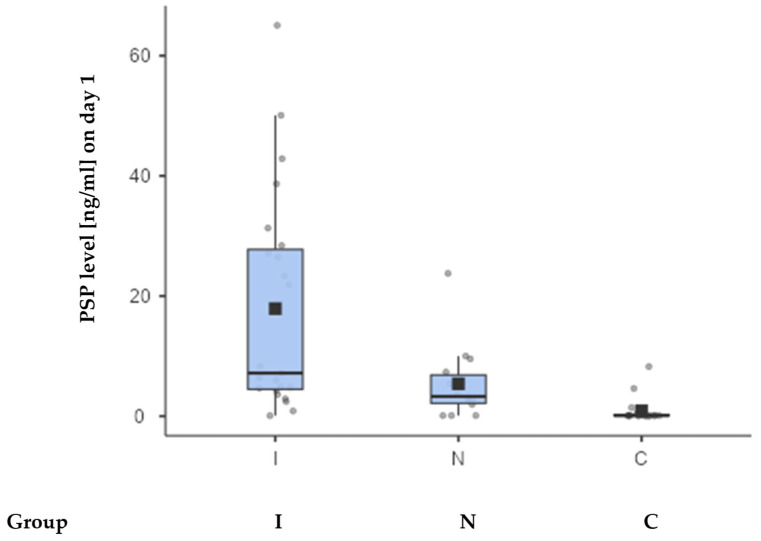
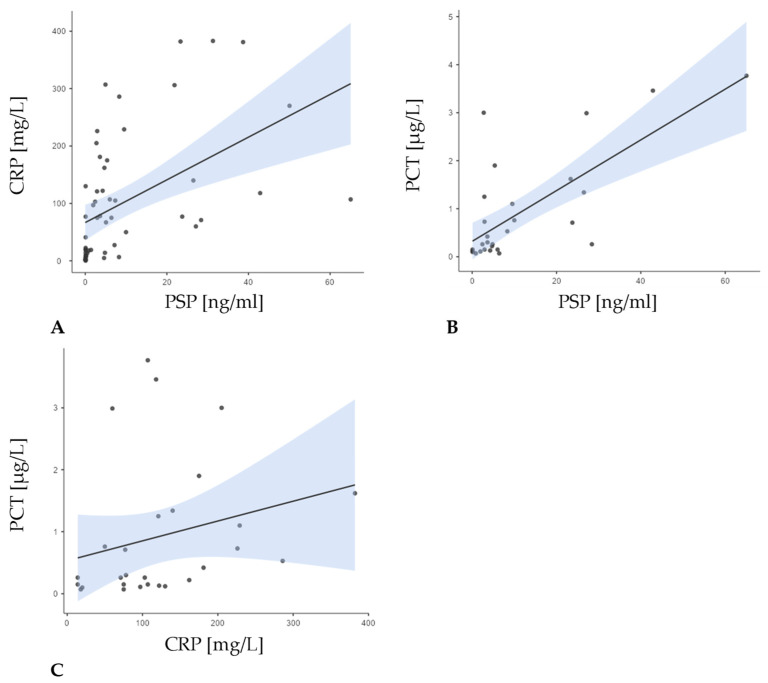
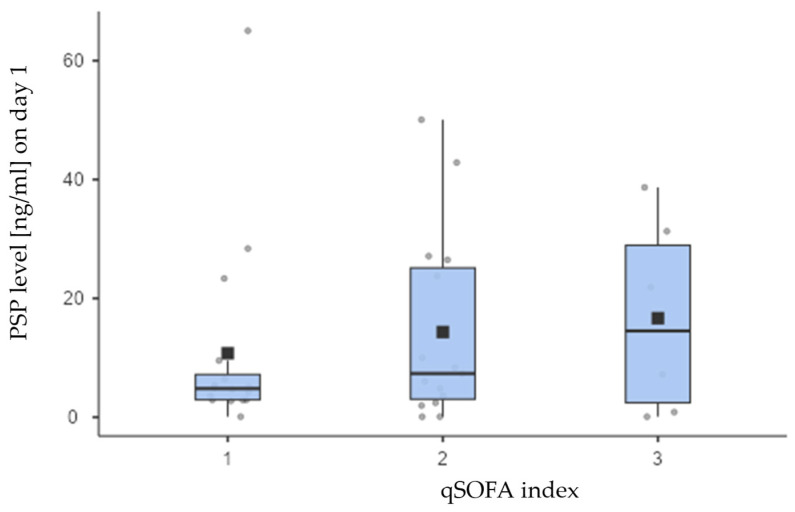
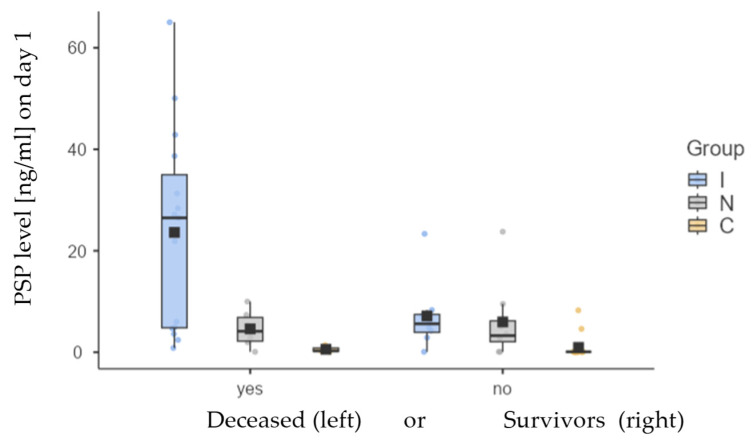
Background/Objectives: In hematological patients receiving treatment for lymphomas, febrile neutropenia (FN) is a serious complication associated with significant morbidity and mortality. This prospective study aimed to evaluate the diagnostic and prognostic value of the novel biomarker presepsin (PSP) in episodes of FN in this specific cohort of patients. Methods: The study enrolled 37 patients with FN and 18 patients with neutropenia without fever as a control group. Patients with FN were divided into two groups: those with confirmed infections and those without them. Various clinical and laboratory parameters were analyzed, including inflammatory and biochemical markers, focusing on implications of PSP. Results: Among patients with FN, 65% had proven infections with significantly higher PSP levels compared to those without infections and control group (p < 0.001). Positive blood cultures were found in 13.5% of all FN episodes. PSP showed greater sensitivity than traditional biomarkers like procalcitonin and C-reactive protein for differentiating septic from non-septic complications. Increased PSP levels at admission suggested a poorer survival prognosis. Each 1 ng/mL increase in PSP correlated with a 5% increase in mortality risk (HR 1.05; p < 0.001), with a one-year mortality rate of 56.7%, underscoring the necessity for better predictive markers. Other markers, including CRP, PCT, IgG, and albumin, were not significantly associated with mortality; however, platelets and qSOFA exhibited borderline significance. Conclusions: PSP is a valuable biomarker for identifying high-risk FN in lymphoma patients and predicting mortality, correlating with infection severity. Larger multi-center studies are needed to validate these findings and optimize PSP's clinical application to improve outcomes.
Keywords: febrile neutropenia; lymphomas; presepsin; prognosis.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures

Similar articles
-
Diagnostic value of levels of presepsin (soluble CD14-subtype) in febrile neutropenia in patients with hematological disorders.J Infect Chemother. 2016 Jul;22(7):466-71. doi: 10.1016/j.jiac.2016.04.002. Epub 2016 May 14. J Infect Chemother. 2016. PMID: 27184936
-
The role of presepsin in pediatric patients with oncological and hematological diseases experiencing febrile neutropenia.Sci Rep. 2023 Apr 20;13(1):6464. doi: 10.1038/s41598-023-33094-2. Sci Rep. 2023. PMID: 37081067 Free PMC article.
-
Analyzing the capability of PSP, PCT and sCD25 to support the diagnosis of infection in cancer patients with febrile neutropenia.Clin Chem Lab Med. 2019 Mar 26;57(4):540-548. doi: 10.1515/cclm-2018-0154. Clin Chem Lab Med. 2019. PMID: 30240355
-
Presepsin in Critical Illness: Current Knowledge and Future Perspectives.Diagnostics (Basel). 2024 Jun 20;14(12):1311. doi: 10.3390/diagnostics14121311. Diagnostics (Basel). 2024. PMID: 38928726 Free PMC article. Review.
-
Novel biomarkers to identify complicated course of febrile neutropenia in hematological patients receiving intensive chemotherapy.Eur J Haematol. 2024 Oct;113(4):392-399. doi: 10.1111/ejh.14264. Epub 2024 Jul 3. Eur J Haematol. 2024. PMID: 38961525 Review.
Cited by
-
Improving Prognostic Accuracy of MASCC Score with Lactate and CRP Measurements in Febrile Neutropenic Patients.Diagnostics (Basel). 2025 Jul 31;15(15):1922. doi: 10.3390/diagnostics15151922. Diagnostics (Basel). 2025. PMID: 40804886 Free PMC article.
References
-
- Flowers C.R., Seidenfeld J., Bow E.J., Karten C., Gleason C., Hawley D.K., Kuderer N.M., Langston A.A., Marr K.A., Rolston K.V., et al. Antimicrobial Prophylaxis and Outpatient Management of Fever and Neutropenia in Adults Treated for Malignancy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013;31:794–810. doi: 10.1200/JCO.2012.45.8661. - DOI - PubMed
-
- Freifeld A.G., Bow E.J., Sepkowitz K.A., Boeckh M.J., Ito J.I., Mullen C.A., Raad I.I., Rolston K.V., Young J.A., Wingard J.R. ; Infectious Diseases Society of America. Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2011;52:e56–e93. doi: 10.1093/cid/cir073. - DOI - PubMed
-
- Baluch A., Shewayish S. Infections in Neutropenic Cancer Patients. Springer; Berlin/Heidelberg, Germany: 2019. Neutropenic Fever; pp. 105–117. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
