

A New Approach for Reconstruction of Severe Horizontal Atrophy of the Posterior Mandible Using "The Honeycomb Technique": A 10-14 Year Follow-Up Retrospective Study
- PMID: 40217697
- PMCID: PMC11989626
- DOI: 10.3390/jcm14072246
A New Approach for Reconstruction of Severe Horizontal Atrophy of the Posterior Mandible Using "The Honeycomb Technique": A 10-14 Year Follow-Up Retrospective Study
Abstract
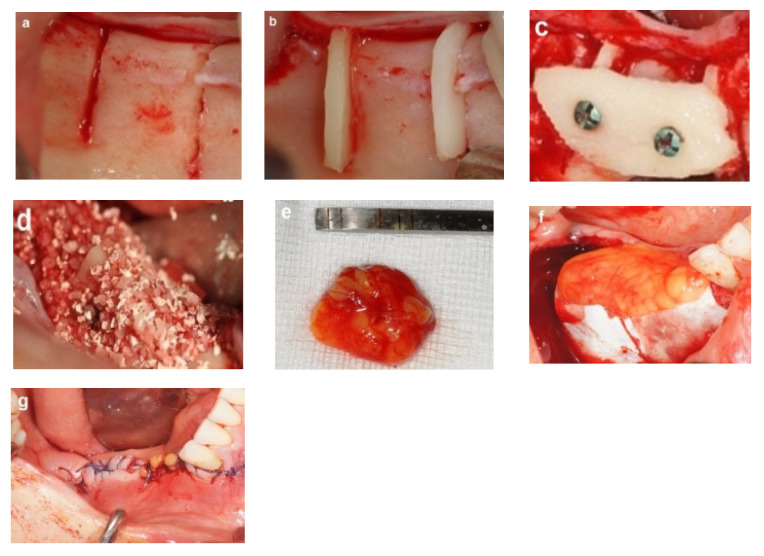
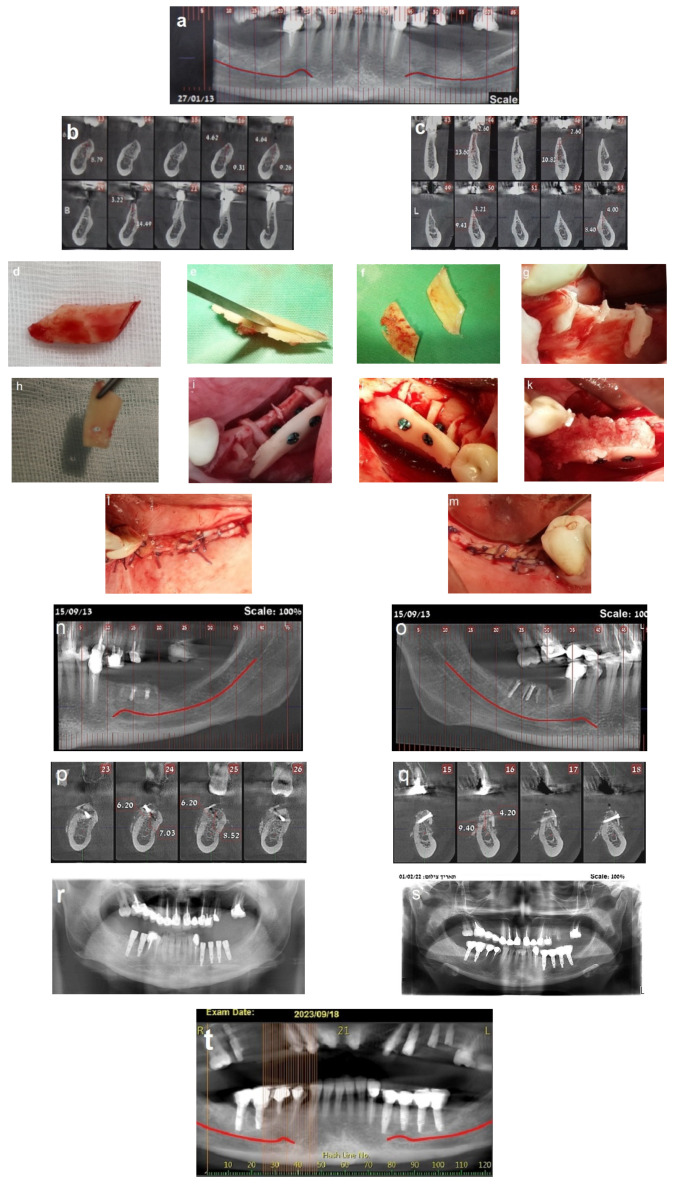
Background: Autogenous bone grafting has long been the standard for augmenting bone prior to implant placement in atrophic ridges. However, innovative techniques are continually sought to enhance outcomes. This study introduces the honeycomb technique for horizontal bone augmentation in edentulous posterior mandibular ridges, presenting the methodology and long-term follow-up results of this novel approach. Methods: This study includes healthy patients with moderate to severe horizontal atrophy in posterior mandibular regions who underwent bone augmentation using the honeycomb technique and were followed up for a period of 10 to 14 years. The patients had orthoradiographs immediately post-surgery and underwent regular clinical and radiographic evaluations. Computed tomography at four months assessed the bone gain, followed by reentry for implant insertion and evaluation of the bone volume and quality. Fixed prosthesis-supported dental implants were placed four months post-insertion. The survival and success of the dental implants were evaluated based on the acceptable clinical and radiographic criteria. Results: A cohort of 23 patients (17 women, 6 men, mean age 47 years) underwent bone augmentation at 39 sites, with follow-up ranging from 10 to 14 years. The procedure demonstrated a 95-100% success rate with minimal morbidity and horizontal bone gain averaging 3-8 mm. Partial graft exposure occurred in two cases but was successfully managed without compromising augmentation. A total of 103 implants were placed in the augmented sites in 37 sites. The long-term survival of the dental implants was confirmed based on clinical and radiographic evaluation, with minimal marginal bone loss observed during the extended follow-up period. Conclusions: The honeycomb technique proves effective in horizontal bone augmentation of atrophic ridges in posterior mandibular defects. The satisfactory long-term outcomes validate its potential as a valuable addition to bone augmentation strategies preceding implant placement.
Keywords: allogenic bone substitute; autogenic bone grafts; bone augmentation; mandibular atrophy; space maintenance.
Conflict of interest statement
The author declares no conflicts of interest.
Figures













References
-
- Felice P., Zucchelli G., Cannizzaro G., Barausse C., Diazzi M., Trullenque-Eriksson A., Esposito M. Immediate, immediate-delayed (6 weeks) and delayed (4 months) post-extractive single implants: 4-month post-loading data from a randomized controlled trial. Eur. J. Oral Implantol. 2016;9:233–247. - PubMed
LinkOut - more resources
Full Text Sources
